
































All:
First, please see my discl0sure here. I'd appreciate this fact not being discussed in open forum, as I value my privacy, but y'all should know.
Now:
I occasionally get requests for an update on my supplement regimen of 4 years ago and my supplement regimen of two years ago, and I'm now following thru'. Once again, I've done more removal of things as stuff has failed to pan out or suddenly appeared to be dangerous than I have in adding new stuff in, along with making a few changes (mostly reductions) in dose, and changing the forms of a couple of items. But things have indeed changed, so here is an update. (I documented some of the changes, and some of the reasons, as I went along in my 2009 regimen post op cit).
As background, please see this post about dietary supplement use in general; this kind of reasoning should inform everyone's judgements about what supplements to take, and why, for them as individuals. Note that I am much more wary about engaging in "Tier 3" speculation than I was back then, and indeed, nearly everything that was on that list at the time has been knocked off by subsequent evidence.
The most important thing you can do as regards all essential vitamins and minerals is to actually use nutrition software to get a handle on your actual dietary intake of these nutrients before deciding what to supplement, tho' this is less of an issue to the extent that your diet is (a) genuinely poor (& thus more likely to actually need 'everything' and not be overdosing on eg Mn, Cu, etc) and (b) you're not on CR (and thus have a lot of 'slop factor' and don't have the specific nutritional risks of CR folk). (Yes, ironically, health-conscious people actually have more need for caution in supplementation, because they often wind up on somewhat restrictive 'health food' regimens that limit the diversity of their nutrient sources, and because, as noted above, it's common for people eating quite well to get almost too much of some nutrients from diet alone, and then add supplements on top of that. Studies show, perversely, that the people who need vitamin supplements the most use fortified cereals the least -- and the converse). A 2-week representative COM crunch of my diet is appended; see also this detailed post on my quotidian diet). Do also make use of the relatively few reliable functional diagnostics for nutrient deficiency, such as serum 25(OH)D3, homocysteine, and MMA.
On this point, let me emphasize the logical corollary which I've spelled out repeatedly but that people keep missing: unless your diet is composed entirely of fries, Coke, and fast-food burgers with the lettuce, ketchup, and tomato thrown out, no one should be taking a full daily dose of any commercial multivitamin. You are absolutely guaranteed to get too much of many nutrients, and to create or exacerbate imbalances in others.
I should also emphasize the other corollary: this is a regimen for a very specific individual: a very healthy, young(ish) CR practitioner with an excellent diet (which I've analyzed extensively, to understand its weaknesses and "excessive" strengths -- see a representative week's average appended to this post). As the links above indicate, a person must customize hir regimen based on hir own diet, and also age, specific risk factors, existing diseases, etc.
So: the regimen (notes on WHY I take various things at the end, when it isn't obvious from the link or other grounds):
UPON WAKING (5 AM or before), w/ green tea 1/3 c pomegranate juice+ 2/3 C diet Dr. Bob [dropped fall 2012; see below]
1/2 tsp (~2.5 1.8 g) CreaPure Creatine monohydrate (do not buy commodity creatine! See below).
1 Prostaphil defined pollen extract
5:50 AM, with coffee green tea [switched fall 2012; see "Quotidian Diet" post]
1000 mg AjiPure L-Lysine
0.5 g Beta-alanine
6:30 AM, breakfast:
[I would be taking Provinols,if I could find them ...]
420 mg Phosphatidylcholine
250 mg Lactoferrin
15 µg vitamin B12 (1/6 of 100 µg tablet)
While scrubbing teeth: 1 drop per eye N-acetyl-L-carnosine eyedrops
10:30 AM, with green tea:
500 mg IP-6
500 mg Inositol (possibly synergistic to IP-6)
11:10 AM, with coffee green tea:
0.5 g Beta-alanine
Brain nutrient (rotating one of: 800 mg piracetam ( why?) (once/wk), pyroglutamate (500 mg, thrice/wk) and ALCAR (125 mg thrice/wk [dropped spring 2013 as a result of (36)])
11:50 AM, with green tea:5001000 mg AjiPure L-Lysine, 500 mg arginine [See my reply to a question from viveutvitas on why I dropped the arginine] (no, these do not interfere with one another's effects for this application).
12:30 PM, lunch:
420 mg Phosphatidylcholine
750 mg taurine
30 mg CoQ10
15 mg Menatetrenone
1 mg Lithium (orotate -- do see note below!)
56 µg Iodine (1/4 of 225 µg, 6 d/wk)
4:30, with coffee green tea or other beverage:
500 mg IP-6
500 mg Inositol (possibly synergistic to IP-6)
5:10, with green tea or other beverage:
0.5-2.5 g Beta-alanine (higher dose when doing resistance training)
1 Prostaphil
5:50, with coffee green tea or other beverage:
1000 mg AjiPure L-Lysine (1.5 g arginine when doing resistance training)
6:30, dinner:
857 IU (average) vitamin D3 (as 1 x 1000 IU softgel, 6 d/wk)
750 mg taurine
15 mg Zn (citrate)
420 mg Phosphatidylcholine [Added 2012/02/14]
10 pm, bed, with green tea or other beverage:
0.5 g Beta-alanine
5 g AjiPure Glycine
314 mg Strontium (citrate)
750 mcg melatonin (as required)
Further on RationalesPomegranate juice: I want SOME source of relatively high-GI sugar without protein or fat to get glucose levels up first thing on rising, and for the possible benefit of taking creatine with a sugar source (tho' it's not at all clear that this is anything like enough glucose to meaningfully affect this, nor that the extra boost to tissue reserves as vs. water coadministration during the loading period is sustained with ongoing administration); I chose pom juice for the many promising-looking studies in disease states, tho' again the dose may be inadequate (studies typically use 1-2 C). Don't blow your bucks on POM Wonderful: Trader Joe's has it reasonably cheap, as does Georgian Nectar (a hard-to-find brand I sometimes find at a local Asian grocery store). I would "look" for brands that aren't syrupy or sickly-sweet, and still have some bitterness and residual granular material; Lakewood has the stuff genuinely fresh-pressed rather than from concentrate, which strikes me as likely preferable, but it's VERY expensive. My preferred brand at the moment is Langers Fresh Pressed (not from concentrate). Nixed the pom juice out of concern about starting my day off with a big blast of sucrose — fall 2012..The diet Dr. Bob is 'cause I like it and it has zero Calories; it's cheaper and to my taste yummier than the brand name original. No, I am not worried about aspartame (or sucralose, for that matter) causing cancer or neurological disease. Indeed, the recent, much-hyped report of increased cancer in aspartame-dosed rodents (3) actually made me less nervous about aspartame: it (a) really didn't clearly show any increased cancer risk (they hyped up non-statistically-significant elevations in incidence of some cancers late in life, but also NS decreases in others), and indeed (b) reported identical survival curves between aspartame-treated and untreated animals (if anything, it looked like females given the highest dose lived LONGER on average than untreated animals); plus, there was massive mortality from inflammatory lung disease and other causes, showing that these people just can't raise healthy mice. Additionally, because aspartame has been on the market for a quarter century and is widely and selectively used, there's now been enough time for both additional direct human and animal research and decades of prospective epidemiology (4,5) showing no ill effects over a wide range of intakes in humans. If you were alarmed by a recent scary-sounding paper in an otherwise-respectable journal,(6) please see this post debunking the junk science on "Direct and indirect cellular effects of aspartame on the brain" by Humphries, Pretorius, and Naudé (5a). However, I am beginning to become concerned about the emerging evidence suggesting long-term dysregulation of glucoregulatory hormones and signaling related to artificial sweetener use, and have cut back quite substantially on consumption of soda and sweetening tea and coffee. This change dates to fall 2012. Later yet (June 2013): cut artificial sweeteners outside of solid food ingredients/condiments (and cut those back) in response to (37).
To read a thoughtful, non-paranoid, non-"it's-just-not-natural!" argument for caution by a reputable and careful scientist, I refer you to Devra Davis' excellent (and disturbing) Secret History of the War on Cancer.
Creatine, beta-alanine, ALCAR, taurine, zinc: I'm ovolacto for my quotidian diet, and am therefore somewhat low on these, and Vegetarian Booster has been discontinued. Plus, I found during a period that I briefly ran out of Veg Booster and had to buy these nutrients (at higher dose) individually, that I felt better on the higher ALCAR and creatine combined with the concomitant R(+)-lipoic acid (which last I took to compensate for the increase in carnitine and teh switch to ALCAR in particular); and, I actually exhibit symptoms of Zn deficiency when I don't, despite a fairly high dietary Zn, presumably due to high dietary copper. More on most of these below. See also this recently-posted thread on supplementation for veg(etari)ans - 2015-02-15. Note that ALCAR, like free choline, can be metabolized into TMAO by gut bacteria ((37) and other references) and appears to promote atherogenesis even in persons with low LDL and other CVD risk factors.
Creatine: As noted, I'm vegetarian, and our intakes and serum levels are lower than omnivores' (from these three sources, it appears that typical omnivorous dietary intake is 1-2 g/d, and some of that will be unabsorbable due to cooking, unlike high-quality supplemental creatine), and trials seem to show that vegetarians'muscles and (on some tasks) brains work better when given a low-dose supplement(18). If you use creatine, insist on a supplement made using CreaPure (a branded raw material manufactured by AlzChem AG (fixed 2012-02-18 -- thanks sdxl) (formerly Degussa AG Trostberg; formerly SKW) but used in several different retail brands). Years ago, Dr. N..... at A0R had raised concerns about contaminants in other creatine manufactrers, but I never looked into it at the time as A0R wasn't marketing it and I wasn't taking it. A while back, however, I bought some creatine from a company that I generally consider to be quite reputable and from whom I often buy commodity-item supplelments, and was disturbed by its very bitter and (surprisingly) soapy taste. I called the company, who dug back thru' their QC procedures and retained sample, insisted that it was fine; I did some digging and found that there are indeed reasons for caution, as outlined in these two very good articles on creatine by Will Brink: "What's in your Creatine?" and "What's Really in Your Supplements? - An Update on Creatine"; see also Alzchem's CreaPure promotional materials. Just recently, see (39). -Edit, 2015-02-15. I proceeded to order some CreaPure-sourced creatine and was surprised that, for the very first time with any creatine supplement, the stuff had absolutely no bitter taste to it: the suspicious supplement had been the first one I'd ever used that had a soapy taste, but every creatine I'd previously used had a mild bitterness to it, which I'd thus assumed to be intrinsic to creatine itself, whereas it now seems it is rather the taste of some impurity. There is no direct evidence that dicyandiamide or dihydrotriazine is harmful -- but why anyone (let alone a life extensionist!) would knowingly put high (relative to likely dietary intakes) levels of organoleptically-detectable impurities of unknown toxicity into hir body to save a few dollars is beyond me.
Also, do read this sensible safety caution about the long-term effects of creatine supplement use (starting just after the paragraph on the effects of caffeine), much of which applies to many other supplements.
I originally thought 1/2 tsp of my creatine delivered ~2.5 g, as per the "Nutrition Facts" panel; upon being asked by bmdelaney, I weighed the stuff, and it's actually ~1.8 g. Annoying, but I'm actually OK with that, as it's closer to typical omnivorous dietary intake is, and thus errs on the side of safety.
Beta-alanine: I was previously taking carnosine, which is possibly anti-senescent cell, possibly anti-mitochondrially-mutant cell, and is deficient in vegetarian diet. However, I've now substituted beta-alanine, for which there is much better evidence of elevation of tissue carnosine levels (and, I happily anecdotally report, seemingly impressive muscle power gains, consistent with the surprisingly large number of clinical trials with the stuff, tho' this wasn't what got me interested originally). One thing to watch out for is the dose: bottle directions often suggest 2 g, 4 x daily, which is the final, ramped-up dose used in the trials; however, this is likely to cause you (as I shame-facedly admit, it caused me) maddening paraesthesia (pins and needles), as explained here. Instead, start at 500 mg 4 x daily, and work your way up as needed or desired; I only take a higher dose on days when I'm doing resistance training.
Prostaphil defined pollen extract: I have an idiopathic urinary urgency; definitely not BPH or bacterial prostatitis, conceivably related to alpha-adrenergic function. This is subjectively very helpful.
Iodine: Getting reliable information on iodine intake is very difficult. As a vegetarian, my intake is probably low, and I do consume a significant amount of cruciferous veggies, which inhibit iodine uptake by the thyroid. I'd strongly caution against using "sea vegetables" as a source, because iodine levels in same can be EXTREMELY high: in particular, kombu kelp can savage your thyroid gland (and see followup on kombu and thyroid risk). Moreover, unfortunately most iodine supplements are kelp-derived and high-dose -- and occasionally unreliable or contaminated with arsenic. The NOW supplement I link above serves my purposes well.
Menatetrenone: I have low BMD typical of natural- and CR-induced low BMI; this is a fracture risk factor, tho' not as much as would be routinely assumed and even diagnosed, because of my overall risk profile: see the new FRAX fracture risk assessment tool developed by the WHO. See also this post on how CR appears to protect bone against age-related decline in bone quality/microarchitecture, for which the available human evidence is now in support, or at least to which it offers no contradiction.(35) Menatetrenone seems promising for CR-related low bone mass, as the actual MASS of bone is constrained by low energy intake, whereas menatetrenone primarily appears to reduce risk by preseving QUALITY -- a more likely viable strategy.Arginine and lysine: these have been found to be surprisingly effective in reducing AGE and AGE-induced complications of diabetes, especially in the kidneys but also apparently in the heart (6-12a). (13) was negative, but the measurement of AGE was in skin, which not be reached by a significant concentration of these nutrients (vs the heart and kidneys, thru' which they would of course travel in the blood when they're taken on an empty stomach) (tho' (11) did find reductions in hexosyllysine), and their conclusion was (reasonably) that "treatment may need to continue for more than 1 year before clinical status improves." [Edit: nixed the arginine, due to concerns raised by viveutvivas]. Sourcing: After first my creatine experience (above), I recently had a quite similar experience with Ajinomoto's AjiPure Glycine: the taste of their product is sweeter and 'cleaner' than any other brand I've used. Because I'm now consuming 3 g of lysine a day, and with the knowledge of the impurities underlying the bitter taste in commodity creatine, and in recollection of the tryptophan-related outbreak of eosinophilia-myalgia syndrome (EMS) in 1989, I've recently (late May 2012) switched from commodity lysine to Ajinomoto's AjiPure L-Lysine.
Provinols: the only authentic red wine concentrate, which I would take if I could find if I could find the darned stuff. Unlike the shaky-to-begin-with-and-now-disproven resveratrol hype, there is a quite solid body of epidemiological evidence of an association between a couple of glasses of wine a day and lower risk of a range of adverse outcomes, including total mortality and dementia. The epidemiology clearly indicates a U-shaped dose-response curve for alcohol consumption and heart disease, with the best outcomes associated with 1-3 drinks/d, and this extends to total mortality in meta-analysis(19); but when broken down into type of alcohol consumed, only wine lowers total mortality and dementia: beer or spirits lower CVD mortality, with no effect on total. (No, despite the use of these findings as a justification for resveratrol supplements, there is no epidemiological evidence favoring red over white). The benefits for total mortality reach a nadir at
Figure 1. Relative risk of total mortality (95% confidence interval) and alcohol intake extracted from 56 curves using fixed- and random-effects models. From (19).
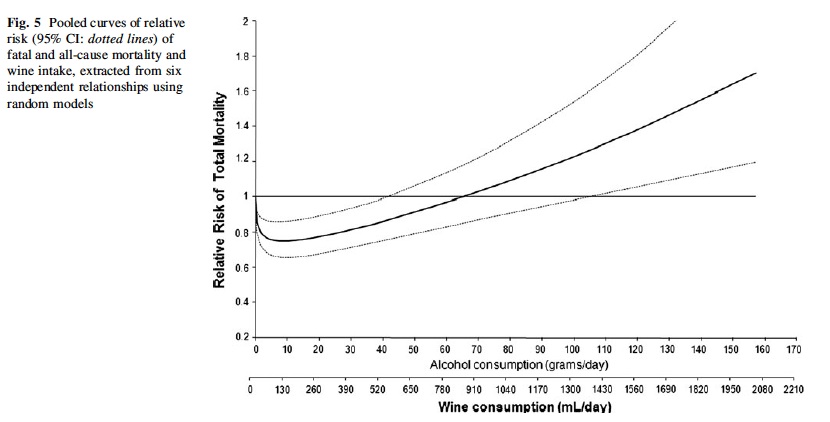
Wine consumption vs. total mortality. From (38).
However, my working hypothesis is that the climbing risk is due to the toxicity of alcohol per se, and that additional benefits might be available from higher intake of the component(s) of wine responsible for these benefits, without the extra Calories and toxicity of drinking the stuff. However, we don't know which component(s) of wine exert these effects, so we should aim for a supplement that is a direct concentrate of the same spectrum of bioactives in actual, fermented wine -- ie, not just resveratrol, nor the grape-seed and/or -skin extract that is often mislabeled "wine extract," and whose polyphenol mix is actually quite different from that in wine, due to complexation and biotransformation that the grapes undergo during fermentation. Seppic in France has done a great deal of work in characterizing these, and still the surface is only barely scratched and we don't know what might do what.
Therefore, I went looking for a genuine concentrate of actual red wine that did not rely on high temperature or extraneous chemicals which might also alter the original mix, and which did not come from China or another country with high levels of industrial contaminants or shady business practices.
I first hit on Provinols, which is a pioneering product in this field, but unfortunately it is damned near impossible to get in the Americas, except in low doses and mixed in with other junk. (Europeans and Turks may be able to get it, however). I was at one time convinced of the authenticity of a product called Wine Rx, but they subsequently failed to document their claims on composition, and moreover, it seems to go vinegary and weird in well less than a year -- not surprising perhaps granted that it was only a 50% extract. So, I wait glumly for the Real Deal.
Phosphatidylcholine: Replaces citicoline and free choline supplements, which may promote atherosclerosis. See also here on supplemental phosphatidylcholine contamination. (Citicoline and carnitine also generate TMAO, NB, and alpha-GPC very likely also does). Note that phosphatidylcholine is only 13% free choline by weight, so eg 420mg of phosphatidylcholine is only ~55 mg free choline (thanks Sillewater!). June 2013: the COM crunch below indicates ~250 mg choline/d from diet; more recent COM crunches indicate ~350. Note that the USDA choline database only includes 630 foods, so one's real intake is certainly higher than what nutrition software indicates -- but don't let this make you overconfident of adequacy. Elevated serum creatine phosphokinase (CPK), aspartate aminotransferase (AST), alanine aminotransferase (ALT), or lactate dehydrogenase (LD) may in some cases indicate choline deficiency, tho' (a) they can be elevated for unrelated reasons, and (b) I'm not clear on how severe one's deficiency has to be before noticeable elevations will occur.
Pyroglutamic acid: VRP, my previous source, has discontinued pyroglutamic acid. I'm very annoyed: this is the SECOND time they've disc. something I use for which they're the only trustworthy source I know, and w/o notice ... And in fact, a quick Google suggests no other source (S*urce N@turals sucks (a couple of flunked consumerlabs.com tests, totally inappropriate tableting of R-LA, other bad behavior), and I don't want arginine pyroglutamate). Damn damn damn! Does anyone know of a reliable source for this supplement?? Or is anyone willing to sell me any sealed, non-expired bottles of VRP's? PM me if so, please).
CoQ10: The evidence on what CR does to CoQ levels in rodents is mixed and hard to interpret, but it's reasonable to think that a CR person's levels might be lower, due to natural downregulation of HmGCoA reductase (the enzyme opposed by statins: statin users have low CoQ, as the products of this enzyme are used to synthesize both cholesterol and CoQ). Whether elevating my serum levels with a pill do me any good is a good question, as is whether any decrease in CoQ might be part of the mechanism of CR ...
Lithium orotate: I just do my best to spread the contents of a 5 mg cap evenly over 5 days. No, this is not the pharmacological dose shown to be neuroprotective in rodents subjected to horrible pharmacological or genetic assault, nor in human disease victims, neither of which are reasonable justification for use (let alone for dosages) in normal, healthy humans. See instead (24), which presents animal studies and a surprisingly large am't of (unfortunately, but of necessity, 'ecological' rather than truly prospective) epidemiology suggesting that Li is an essential nutrient, with an 'RDA' of ~ 1 mg, whose presence in the water is linked to having a much happier (less violent, criminal, suicidal, and generally "crazy") population; see also (25), quite recently, in Japan. More recently, this same Japanese study seems to have documented a non-sneezable increase in life expectancy in the higher-Li-water communities.(32) The source I used to use (guess who  ?) has unfortunately quit the market, and most of the alternatives are fly-by-night operations; I would probably recommend VRP. Whatever the merits of the orotate salt specifically (and I'm skeptical, esp at this dose), there's a good chance that even these guys don't have real Li orotate: most of the material out there is just the chloride or carbonate in a blend with orotic acid in the suitable proportions; unfortunately, there's no positive test for the compound per se, and so you have to do a series of negative tests to exclude chloride and carbonate, and almost no one does this. In my former career I went looking for the real deal, and couldn't find it ANY materials suppliers that had it, despite their claims, and it had to be contract manufactured by a company that specializes in true chelates (and then, they dropped it).
?) has unfortunately quit the market, and most of the alternatives are fly-by-night operations; I would probably recommend VRP. Whatever the merits of the orotate salt specifically (and I'm skeptical, esp at this dose), there's a good chance that even these guys don't have real Li orotate: most of the material out there is just the chloride or carbonate in a blend with orotic acid in the suitable proportions; unfortunately, there's no positive test for the compound per se, and so you have to do a series of negative tests to exclude chloride and carbonate, and almost no one does this. In my former career I went looking for the real deal, and couldn't find it ANY materials suppliers that had it, despite their claims, and it had to be contract manufactured by a company that specializes in true chelates (and then, they dropped it).
Zinc: my regular diet includes what should be quite adequate zinc, but my dietary copper intake is so high I get (copper-induced secondary zinc deficiency if I don't supplement (click on the "Research" tab; most people are more likely to have the converse problem). This was mildly symptomatic for much of the year for several years (Beau's lines (more usually associated with iron deficiency), cracking fingertip skin, inability to taste zinc sulphate heptahydrate solution) when I don't, despite a fairly high dietary Zn, presumably due to high dietary copper), and even the 7 mg/d in the Veg Booster wan't quite enough to keep it at bay.
Vitamin D3: A recent meta-analysis of prospective studies posted by Sillewater(17) provides the best evidence on optimal serum levels:
Quote
We used nonparametric ("highest compared with lowest" categories) and parametric (>2 categories) statistical models to evaluate associations of 25-hydroxyvitamin D [25(OH)D] serum concentrations and mortality in observational studies among general populations ... [in data pooled from] studies that contained data on relative risks (RRs) for mortality for different 25(OH)D concentrations, which included a corresponding measure of uncertainty, and this yielded 14 prospective cohort studies that involved 5562 deaths out of 62,548 individuals. We applied log-transformed RRs and CIs, adjusted for the maximal number of confounding variables. ...
In the parametric model, the estimated summary RRs (95% CI) of mortality were 0.86 (0.82, 0.91), 0.77 (0.70, 0.84), and 0.69 (0.60, 0.78) for individuals with an increase of 12.5, 25, and 50 nmol 25(OH)D serum values/L, respectively, from a median reference category of ∼27.5 nmol/L. [MR: ie, the risk of mortality relative to an absolute serum value of ∼27.5 nmol/L (11 ng/mL) was .86 for individuals with a serum value of 40 nmol/L (16 ng/mL) 0.77 for individuals with a serum value of 52.5 nmol/L (21 ng/mL), and 0.69 for individuals with a serum value of 77.5 nmol/L (31 ng/mL)].
There was, however, no significant decrease in mortality when an increase of ∼87.5 nmol/L above the reference category occurred [ie, the mortality risk for an absolute value of 115 nmol/L (46 ng/mL) is not significantly different from having a frankly deficient serum value of ∼27.5 nmol/L (11 ng/mL): you're better off at or around 31 ng/mL].
Conclusion: Data suggest a nonlinear decrease in mortality risk as circulating 25(OH)D increases, with optimal concentrations ∼75-87.5 nmol/L [30-46 ng/mL]."(17)
You can see this in their Figure, which is nominally U-shaped, with the sweet spot at ~31 ng/mL, although the CIs don't rule out the possibility that mortality merely FLATTENS at 31 ng/mL and above, rather than reaching a true trough there with risks getting worse at higher values:

Caption: "Summary nonlinear dose-response relation (dotted lines: 95% CI) from the best-fitting random-effects model, between an increase in the concentration of 25(OH)D (ng/mL) with respect to reference values and overall mortality RR. ... Summary RR = exp (20.0850x + 0.00175x2). The lower x axis indicates the absolute 25(OH)D values. Note that 27.5 nmol/L is the median value of the reference categories of our included studies. To convert the values of 25(OH)D to ng/L, divide by 2.496. 25(OH)D, 25-hydroxyvitamin D."
At 1000-1200 IU/d, I have consistently had a little over 40 ng/dL serum 25(OH)D3. Thus, I've cut back to beneath the low end of that range, and will reasess even that dose if my levels don't drop.
Taurine: Absent in vegetarian diet; significant, altho' not ideal, data that it reduces the risk of CVD and other mortality.(33) NB that the EPA/DHA and taurine content of fish and seafood are major confounders to drawing inferences about observed benefits of fish consumption in epidemiological studies; while there are controlled trials showing lower risk of a second heart attack or major cardiovascular events with EPA/DHA supplements or extra ALA, there is as yet no real equivalent with taurine. In in Japan, the average intake appears to be 225 mg/d in males and 162 in females, with the highest intakes >1000 mg.(34)
Glycine: mostly for soundness of sleep (16). I've switched over to their AjiPure Glycine Powder, for reasons discussed in the discussion of lysine, above.
Strontium: As noted, I have low BMD typical of natural- and CR-induced low BMI; strontium is one of the best-documented supplements on the planet, having been shown in multiple clinical trials (of post- or peripausal women, NB, whose bone loss is for very different reasons and is associated with decay of bone architecture) to actively increase bone formation, raise or maintain BMD, and reduce fracture risk.
Melatonin: for sleep when stressed, wide awake, or jetlagged. 300 mcg is sufficient to raise levels to normal physiological youthful ones and apparently works as well as higher doses ((22,23), and see (21)) and doesn't produce the 'hangover' sleepiness sometimes seen with the supraphysiological 3 mg (and up) doses that became ubiquitous thanks to the recommendation of the once-notorious Melatonin Miracle.
And with that melatonin discussion, I symbolically put this thing to bed -- for another long sleep!
-Michael
Representative 2-week CRON-O-Meter:
General
===========================================
Energy | 1731.4 kcal 271%
Protein | 79.3 g 165%
Carbs | 188.2 g 63%
Fiber | 67.3 g 224%
Starch | 2.2 g
Sugars | 59.1 g
Fat | 84.0 g 382%
Alcohol | 9.3 g
Caffeine | 2.8 mg
Water | 1879.8 g 125%
Ash | 21.1 g
Vitamins (86%)
===========================================
Vitamin A | 31538.5 IU 1051%
Retinol | 105.2 µg
Alpha-carotene | 1444.6 µg
Beta-carotene | 17592.6 µg
Beta-cryptoxanthin | 23.5 µg
Lycopene | 12416.8 µg
Lutein+Zeaxanthin | 25686.3 µg
Folate | 1164.0 µg 233%
B1 (Thiamine) | 2.7 mg 227%
B2 (Riboflavin) | 2.5 mg 195%
B3 (Niacin) | 26.5 mg 166%
B5 (Pantothenic Acid)| 12.0 mg 240%
B6 (Pyridoxine) | 3.8 mg 224%
B12 (Cyanocobalamin) | 1.3 µg 55%
Vitamin C | 558.1 mg 620%
Vitamin D | 65.4 IU 16%
Vitamin E | 27.2 mg 181%
Beta Tocopherol | 0.2 mg
Delta Tocopherol | 0.0 mg
Gamma Tocopherol | 5.8 mg
Vitamin K | 1256.1 µg 1047%
Biotin | 0.0 µg 0%
Choline | 248.4 mg 45%
Minerals (100%)
===========================================
Calcium | 1214.6 mg 121%
Chromium | 0.0 µg 0%
Copper | 3.4 mg 377%
Fluoride | 92.6 µg
Iron | 21.8 mg 273%
Magnesium | 659.5 mg 157%
Manganese | 11.0 mg 480%
Phosphorus | 1700.8 mg 243%
Potassium | 6508.3 mg 138%
Selenium | 66.9 µg 122%
Sodium | 1235.1 mg 95%
Zinc | 14.5 mg 132%
Amino Acids (93%)
===========================================
ALA | 3.2 g
ARG | 4.9 g
ASP | 6.8 g
CYS | 1.0 g 70%
GLU | 11.5 g
GLY | 2.6 g
HIS | 1.6 g 151%
HYP | 0.0 g
ILE | 2.8 g 194%
LEU | 4.5 g 140%
LYS | 3.7 g 125%
MET | 1.1 g 74%
PHE | 3.0 g 117%
PRO | 3.1 g
SER | 3.1 g
THR | 2.5 g 165%
TRP | 0.8 g 220%
TYR | 2.1 g 85%
VAL | 3.4 g 1116%
Lipids (55%)
===========================================
Saturated | 9.9 g
Monounsaturated | 50.8 g
Polyunsaturated | 17.3 g
Omega-3 | 4.8 g 121%
Omega-6 | 12.5 g
Trans-Fats | 0.0 g
Cholesterol | 27.0 mg 9%
Phytosterol | 199.5 mg
References
3. Soffritti M, Belpoggi F, Degli Esposti D, Lambertini L, Tibaldi E, Rigano A. First experimental demonstration of the multipotential carcinogenic effects of aspartame administered in the feed to Sprague-Dawley rats. Environ Health Perspect. 2006 Mar;114(3):379-85. PMID: 16507461 [PubMed - indexed for MEDLINE]
4. Gallus S, Scotti L, Negri E, Talamini R, Franceschi S, Montella M, Giacosa A, Dal Maso L, La Vecchia C. Artificial sweeteners and cancer risk in a network of case-control studies. Ann Oncol. 2007 Jan;18(1):40-4. Epub 2006 Oct 16. PMID: 17043096 [PubMed - indexed for MEDLINE]
5. Lim U, Subar AF, Mouw T, Hartge P, Morton LM, Stolzenberg-Solomon R, Campbell D, Hollenbeck AR, Schatzkin A. Consumption of aspartame-containing beverages and incidence of hematopoietic and brain malignancies. Cancer Epidemiol Biomarkers Prev. 2006 Sep;15(9):1654-9. PMID: 16985027 [PubMed - indexed for MEDLINE]
5a. Humphries P, Pretorius E, Naudé H. Abstract Direct and indirect cellular effects of aspartame on the brain. Eur J Clin Nutr. 2008 Apr;62(4):451-62. Epub 2007 Aug 8. PMID: 17684524 [PubMed - in process] http://www.nature.co...866a.pdf
6: Geogescu A, Popov D. Age-dependent accumulation of advanced glycatin endproducts is accelerated in combined hyperlipidemia and hyperglycemia, a process attenuated by L-arginine. J Amer Aging Assoc. 2000 Jan;23(1):23-30.
6a. Lubec B, Golej J, Marx M, Weninger M, Hoeger H. L-arginine reduces kidney lipid peroxidation, glycoxidation and collagen accumulation in the aging NMRI mouse. Ren Physiol Biochem. 1995 Mar-Apr;18(2):97-102. PMID: 7539539 [PubMed - indexed for MEDLINE]
7. Weninger M, Xi Z, Lubec B, Szalay S, Hoger H, Lubec G. L-arginine reduces glomerular basement membrane collagen N epsilon-carboxymethyllysine in the diabetic db/db mouse. Nephron. 1992;62(1):80-3. PMID: 1436297
8. Radner W, Hoger H, Lubec B, Salzer H, Lubec G. L-arginine reduces kidney collagen accumulation and N-epsilon-(carboxymethyl)lysine in the aging NMRI-mouse. J Gerontol. 1994 Mar;49(2):M44-6. PMID: 8126351 [PubMed - indexed for MEDLINE]
9. Sensi M, De Rossi MG, Celi FS, Cristina A, Rosati C, Perrett D, Andreani D, Di Mario U. D-lysine reduces the non-enzymatic glycation of proteins in experimental diabetes mellitus in rats. Diabetologia. 1993 Sep;36(9):797-801. PMID: 8405749 [PubMed - indexed for MEDLINE]
10. Khaidar A, Marx M, Lubec B, Lubec G. L-arginine reduces heart collagen accumulation in the diabetic db/db mouse. Circulation. 1994 Jul;90(1):479-83. PMID: 8026034 [PubMed - indexed for MEDLINE]
11. Lubec G, Vierhapper H, Bailey AJ, Damjancic P, Fasching P,Sims TJ, Kampel1 D, Popow C, Bartosch B. Influence of L-arginine on glucose mediated collagen cross link precursors in patients with diabetes mellitus. Amino Acids. 1991 Feb;1(1):73 – 80.
12. Jyothirmayi GN, Modak R, Reddi AS. L-lysine reduces nonenzymatic glycation of glomerular basement membrane collagen and albuminuria in diabetic rats. Nephron. 2001 Feb;87(2):148-54. PMID: 11244310 [PubMed - indexed for MEDLINE]
12a: Sulochana KN, Punitham R, Ramakrishnan S. Beneficial effect of lysine and amino acids on cataractogenesis in experimental diabetes through possible antiglycation of lens proteins. Exp Eye Res. 1998 Nov;67(5):597-601. PubMed PMID: 9878222.
13. Contreras I, Reiser KM, Martinez N, Giansante E, Lopez T, Suarez N, Postalian S, Molina M, Gonzalez F, Sanchez MR, Camejo M, Blanco MC. Effects of aspirin or basic amino acids on collagen cross-links and complications in NIDDM. Diabetes Care. 1997 May;20(5):832-5. PMID: 9135951
16: Inagawa K, Hiraoka T, Kohda T, Yamadera W, Takahashi M. Subjective effects of glycine ingestion before bedtime on sleep quality. Sleep and Biological Rhythms.2006 Fe;4(1):75-7.
17. Zittermann A, Iodice S, Pilz S, Grant WB, Bagnardi V, Gandini S. Vitamin D deficiency and mortality risk in the general population: a meta-analysis of prospective cohort studies. Am J Clin Nutr. 2011 Dec 14. [Epub ahead of print] PubMed PMID: 22170374.
18: Rae C, Digney AL, McEwan SR, Bates TC. Oral creatine monohydrate supplementation improves brain performance: a double-blind, placebo-controlled, cross-over trial. Proc Biol Sci. 2003 Oct 22;270(1529):2147-50. PubMed PMID: 14561278; PubMed Central PMCID: PMC1691485.
19. Di Castelnuovo A, Costanzo S, Bagnardi V, Donati MB, Iacoviello L, de Gaetano G. Alcohol dosing and total mortality in men and women: an updated meta-analysisof 34 prospective studies. Arch Intern Med. 2006 Dec 11-25;166(22):2437-45. PubMed PMID: 17159008.
20. Streppel MT, Ocké MC, Boshuizen HC, Kok FJ, Kromhout D. Long-term wine consumption is related tocardiovascular mortality and life expectancy independently of moderate alcohol intake: the Zutphen Study. J Epidemiol Community Health. 2009 Jul;63(7):534-40. PubMed PMID: 19406740.
21: Brzezinski A, Vangel MG, Wurtman RJ, Norrie G, Zhdanova I, Ben-Shushan A, Ford I. Effects of exogenous melatonin on sleep: a meta-analysis. Sleep Med Rev. 2005 Feb;9(1):41-50. PubMed PMID: 15649737.
22: Zhdanova IV, Wurtman RJ, Morabito C, Piotrovska VR, Lynch HJ. Effects of low oral doses of melatonin, given 2-4 hours before habitual bedtime, on sleep in normal young humans. Sleep. 1996 Jun;19(5):423-31. PubMed PMID: 8843534.
23: Zhdanova IV, Wurtman RJ, Lynch HJ, Ives JR, Dollins AB, Morabito C, Matheson JK, Schomer DL. Sleep-inducing effects of low doses of melatonin ingested in the evening. Clin Pharmacol Ther. 1995 May;57(5):552-8. PubMed PMID: 7768078.
24. Schrauzer GN. Lithium: occurrence, dietary intakes, nutritional essentiality. J Am Coll Nutr. 2002 Feb ;21 (1):14-21. PMID 11838882
25. Ohgami H, Terao T, Shiotsuki I, Ishii N, Iwata N. Lithium levels in drinking water and risk of suicide. Br J Psychiatry. 2009 May ;194 (5):464-5; discussion 446. PMID 19407280
32. Zarse K, Terao T, Tian J, Iwata N, Ishii N, Ristow M. Low-dose lithium uptake promotes longevity in humans and metazoans. Eur J Nutr. 2011 Feb 8. [Epub ahead of print] PubMed PMID: 21301855.
32: Yamori Y, Liu L, Mori M, Sagara M, Murakami S, Nara Y, Mizushima S. Taurine as
the nutritional factor for the longevity of the Japanese revealed by a world-wide
epidemiological survey. Adv Exp Med Biol. 2009;643:13-25. PubMed PMID: 19239132.
33: Laura Della Corte (Editor), Ryan J. Huxtable (Editor), Giampietro Sgaragli (Editor), Keith F. Tipton (Editor). Taurine 4: Taurine and Excitable Tissues: Taurine and Excitable Tissues No. 4 (Advances in Experimental Medicine and Biology Volume 483). ISBN (9780306464478) . See here (Fig. 3) and here (Fig. 1).
35: Villareal DT, Kotyk JJ, Armamento-Villareal RC, Kenguva V, Seaman P, Shahar A, Wald MJ, Kleerekoper M, Fontana L. Reduced bone mineral density is not associated with significantly reduced bone quality in men and women practicing long-term calorie restriction with adequate nutrition. Aging Cell. 2011 Feb;10(1):96-102. doi: 10.1111/j.1474-9726.2010.00643.x. Epub 2010 Nov 15. PubMed PMID: 20969721.
36. Koeth RA, Wang Z, Levison BS, Buffa JA, Org E, Sheehy BT, Britt EB, Fu X, Wu Y, Li L, Smith JD, Didonato JA, Chen J, Li H, Wu GD, Lewis JD, Warrier M, Brown JM, Krauss RM, Tang WH, Bushman FD, Lusis AJ, Hazen SL. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013 May;19(5):576-85. doi: 10.1038/nm.3145. Epub 2013 Apr 7. PubMed PMID: 23563705; PubMed Central PMCID: PMC3650111.
37. Pepino MY, Tiemann CD, Patterson BW, Wice BM, Klein S. Sucralose Affects Glycemic and Hormonal Responses to an Oral Glucose Load. Diabetes Care. 2013 Apr 30. [Epub ahead of print] PubMed PMID: 23633524.
38. Costanzo S, Di Castelnuovo A, Donati MB, Iacoviello L, de Gaetano G. Wine, beer or spirit drinking in relation to fatal and non-fatal cardiovascular events: a meta-analysis. Eur J Epidemiol. 2011 Nov;26(11):833-50. doi: 10.1007/s10654-011-9631-0. Epub 2011 Nov 11. PubMed PMID: 22076059.
39 Sabrina Moret; Annalisa Prevarin; Franco Tubaro. Levels of creatine, organic contaminants and heavy metals in creatine dietary supplements. Food Chemistry 2011 Jun;126(3): 1232-1238 DOI: 10.1016/j.foodchem.2010.12.028

Edited by Michael, 28 June 2016 - 02:26 AM.



























