































 3 votes
3 votes
Geroprotector review: Metformin
metformin geroprotector lifespan aging drug
Geroprotector review: Metformin
This article
- is a summary - The full version can be downloaded here:  Geroprotector review - Metformin.pdf (1.22MB)
Geroprotector review - Metformin.pdf (1.22MB)
downloads: 4097
- is a 2017 (spring) update - See here for a 2011 article on metformin by the Author.
- is solely for information purposes, not a substitute for professional medical or dietary advice. The provisos of the LongeCity user agreement apply.
Introduction
Metformin (1,1-dimethylbiguanide) is an oral drug used for the treatment of type 2 diabetes and polycystic ovary syndrome (PCOS). It belongs to a category of drugs known as biguanides but metformin is the only one of this class that remains in clinical use. Metformin is, unless contra-indicated, the first line treatment for type 2 diabetes to which other drugs can be added if needed to achieve the desired level of blood sugar control. Metformin has been included in the World Health Organization’s (WHO) list of essential medicines. Nearly 120 million metformin prescriptions are issued worldwide each year making metformin one of the most sold drugs. Metformin is so popular because it’s relatively safe, efficient, and costs only cents per dose.
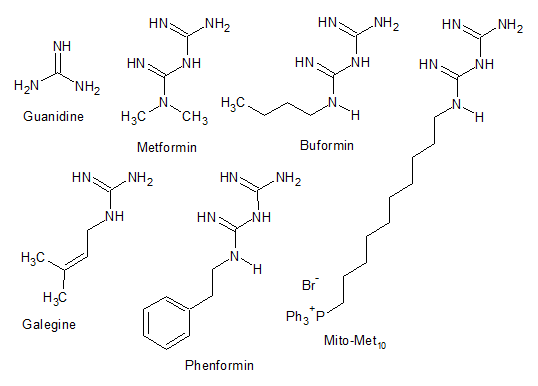
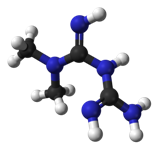
Figure 1 Some of the molecules mentioned in this article. Notice that all molecules share the same guanidine moiety.
During the Middle Ages physicians prescribed Galega officinalis, better known as goat’s rue, the French lilac, Italian fitch, Spanish sanfoin or false indigo, to treat the intense urination in people suffering from type 2 diabetes (Fig. 2).
 (click to enlarge)
(click to enlarge)
Figure 2 Galega officinalis. Credit JoJan on Wikimedia Commons
The active ingredient in this plant is galegine or isoamylene guanidine but this is too toxic for therapeutic use. In fact the name goat’s rue refers to the fact that this plant can be deadly when eaten by grazing sheep or goats. In 1926 two synthetic molecules were discovered that have chemical similarity to the active ingredient of G. officinalis, termed synthalins A and B. These two synthetic molecules were better tolerated and more efficient but still had some toxicity. The discovery of insulin eventually lead to a discontinuation of the synthalins in the early 1930s. In 1929 several biguanides were synthesised including metformin but it was not until 1956 until the antidiabetic properties of these compounds would be investigated by French researcher Jean Sterne. Sterne proposed the name ‘Glucophage’, which is still a brand name of metformin until this day. In the following years two more biguanides were developed: buformin and phenformin. Buformin and phenformin have been withdrawn from the market due to concerns about the increased risk of lactic acidosis (see below). The concern about lactic acidosis kept metformin from the US market until it was finally approved in 1995.
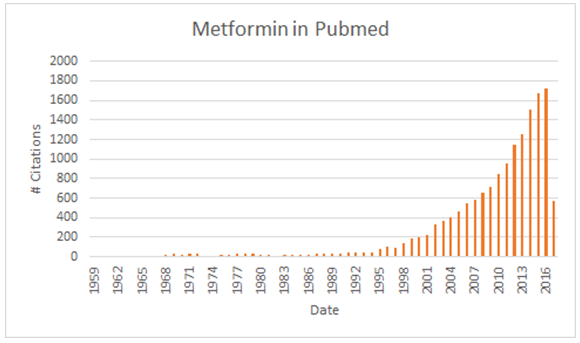
The first paper in Pubmed that contains the search term “metformin” was published in 1959. Remarkably, it took until 1991 before the milestone of 50 papers/year was reached. Just 5 years later this had grown to 100 papers a year and from then on it kept growing, reaching 1717 papers in 2016 (Fig. 3). That’s almost 5 new papers every day!
 (click to enlarge)
(click to enlarge)
Figure 3 Metformin citations in Pubmed. Search conducted on 1st April, 2017.
Metformin’s effects on lifespan
In the full version (see PDF) all available data on lifespan have been included in three tables. Here we just present a short summary of the most important findings.
simple organisms: Metformin extended chronological lifespan in two yeast studies but not in a third one. Three studies report lifespan extension by metformin in the roundworm and one reports lifespan extension by buformin. Metformin also improved several markers of healthspan in worms such as locomotory activity and age-related degradation of the cuticle (= the ‘skin’ of the worm). One interesting result in worms was the finding that metformin actually reduced lifespan in worms grown in bacteria-free conditions. The authors demonstrated that metformin influenced the metabolism of bacteria on which these worms live resulting in a decrease in dietary methionine. No effect of metformin was found on lifespan in fruit flies - at high dosages lifespan actually tended to decrease. However metformin rescued the shortened lifespan of amyloid-β overexpressing flies. Amyloid-β is an aggregation-prone protein that forms the plaques found in the brain of Alzheimer’s disease patients. Furthermore, metformin reduced mortality in 'obese' flies infected with a mold (R. oryzae). Metformin however did not improve survival in 'obese' non-infected flies even though it did induce weight loss. Finally, metformin extended lifespan in crickets.
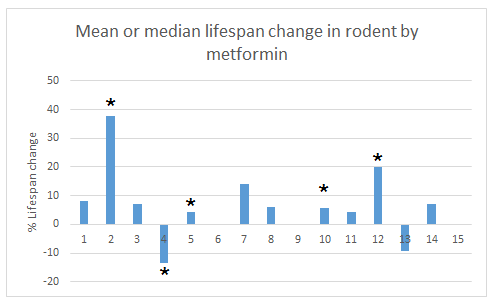
mammals: Phenformin extended lifespan in female mice and female rats. One study found that buformin extended lifespan in female rats. Nine studies have been published examining the effect of metformin on lifespan in rodents. As can be seen in figure 4 metformin largely had a positive effect on mean or median lifespans. Though one study found a significant decrease of 13.4% in male 129/Sv mice. Maximum lifespan was also extended in several studies. Anisimov and colleagues have also demonstrated that metformin reduced the rate of aging in multiple studies. Metformin extended median lifespan of male UM-HET3 mice by 7% (although this was not significant) in the Interventions Testing Program of the NIA. Metformin had no effect on lifespan in this study.
 (click to enlarge)
(click to enlarge)
Figure 4 Mean or median changes in lifespan by metformin in rodents. The asterisks indicate significance by whatever criteria applied in the original paper. 1-15 refers to the order in which the metformin data have been tabled in the full text version. One datapoint, a 14.4% decrease in lifespan in male C57BL/6 mice was censored because the dose used (1% of diet) was toxic while lifespan was extended in that same study by the low (0.1%) dose.
The effect of metformin on lifespan may be age-, gender-, strain-, and dose-dependent (see full text). The combination of metformin and rapamycin may extend lifespan more than either drug alone. Interestingly, long-term rapamycin treatment causes some side effects (glucose intolerance and hyperlipidemia) which could be improved by metformin treatment.
Calorie restriction (CR) is the most robust experimental method to increase lifespan. It has been demonstrated to increase lifespan in a wide variety of model organisms from yeast to monkeys. Stephen Spindler and colleagues tested the effect of metformin on gene expression in the livers of mice. Eight weeks of metformin treatment reproduced 75% of the gene expression changes observed in long term calorie restriction (CR). In comparison eight weeks of CR only reproduced 71% of gene expression changes observed in long term CR. These data support the idea that metformin may work as a CR mimetic.
Multiple trials show that metformin lowers all cause mortality in type 2 diabetes patients when compared to other interventions (see full text, table 3). 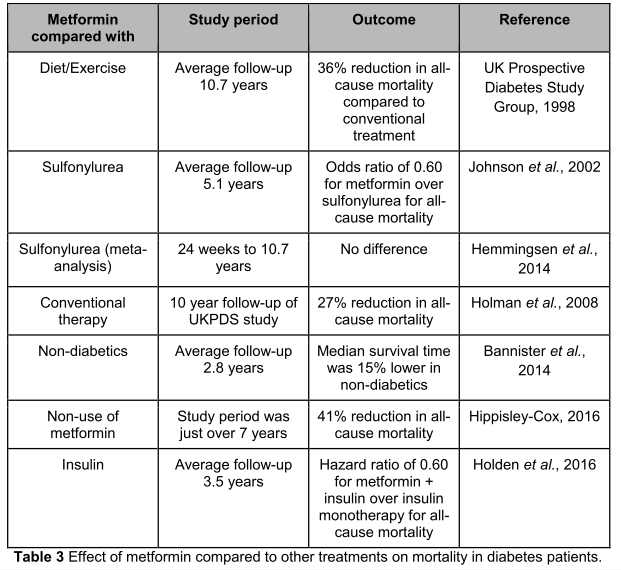 (click to enlarge)
(click to enlarge)
Table: metformin trials & mortality
Surprisingly enough, Bannister and colleagues found that mortality in type 2 diabetes patients treated with metformin was lower than in non-diabetic controls.
The Targeting Aging with Metformin (TAME) trial will enrol roughly 3,000 elderly (65-79 years old). This placebo-controlled, randomized clinical trial will investigate the effect of metformin on a composite outcome that includes cardiovascular events, cancer, dementia, and mortality.
The Me.Me.Me trial is a phase III randomized controlled trial in which the effect of metformin-treatment on the risk for age-related non-communicable chronic diseases will be investigated in people who suffer from metabolic syndrome but are otherwise healthy.
Protective effects of metformin on diseases
Cancer
Various animal studies have shown that metformin reduces spontaneous and induced (such as by exposure to carcinogens) cancers as well as reducing cancer incidence in animals that are genetically susceptible to cancer. Furthermore, metformin sensitizes cancer cells to radiation- or chemotherapy-induced cell death and may simultaneously protect healthy cells from damage from the cancer treatment (see full text).
Multiple cohort and case-control studies in humans show that metformin use by diabetics is associated with a lower risk of cancer. Indeed, when a meta-analysis is done only including cohort and case-control studies than metformin use is associated with a lower cancer risk. However, randomized placebo-controlled clinical trials generally fail to find any benefit from metformin and when they are included in meta-analyses then the beneficial effect of metformin against cancer disappears. Multiple clinical studies are currently ongoing that will hopefully provide better evidence about metformin’s effectiveness in treating cancer.
Lewis Cantley, director of the Cancer Center at Beth Israel Deaconess Medical Center, told Gary Taubes in an interview that “Metformin may have already saved more people from cancer deaths than any drug in history”.
Cardiovascular disease
Metformin treatment improved several classical measures of cardiovascular health including reductions in triglycerides, total cholesterol, very low-density lipoprotein (VLDL) cholesterol, low-density lipoprotein (LDL) cholesterol, lipoprotein(a), and Apo B levels (see full text).
Metformin treatment significantly reduced the progression of aortic atherosclerosis in a rabbit model. Multiple rodent studies have demonstrated that metformin reduces infarct size and ameliorates heart failure after an experimentally-induced heart attack (see full text). Most famously, the UK Prospective Diabetes Study (UKPDS) found a significant reduction in myocardial infarction in type 2 diabetes patients using metformin.
Multiple rodent studies also demonstrate significant benefit from metformin therapy on experimental-induced stroke including reductions in infarct size, neurological symptoms and improvements in the formation of new blood vessels (see full text). Cheng and colleagues used data from the Taiwan National Health Research Institute database to investigate the effect of metformin use on stroke risk in diabetic patients. After a 4-year follow up, metformin use was associated with a significant decrease in the risk for stroke (Hazard Ratio: 0.468). Mima and colleagues found that neurological severity of stroke was lower in type 2 diabetes patients treated with metformin compared to those on other treatments.
Other diseases
Finally, there’s some evidence for a beneficial effect from metformin in various autoimmune diseases (rheumatoid arthritis, multiple sclerosis, inflammatory bowel disease, and lupus), eye diseases (open-angle glaucoma and cataracts), allergic diseases (psoriasis and asthma), anti-fibrotic (lung and liver), non-alcoholic fatty liver disease, infectious diseases (tuberculosis and Clostridium difficile), intervertebral disc degeneration, Huntington’s disease, cyclic edema, and seizures (see full text).
Metformin had a negative effect on disease onset and progression in an amyotrophic lateral sclerosis (ALS) mouse model.
Mechanisms of metformin
 (click to enlarge)
(click to enlarge)
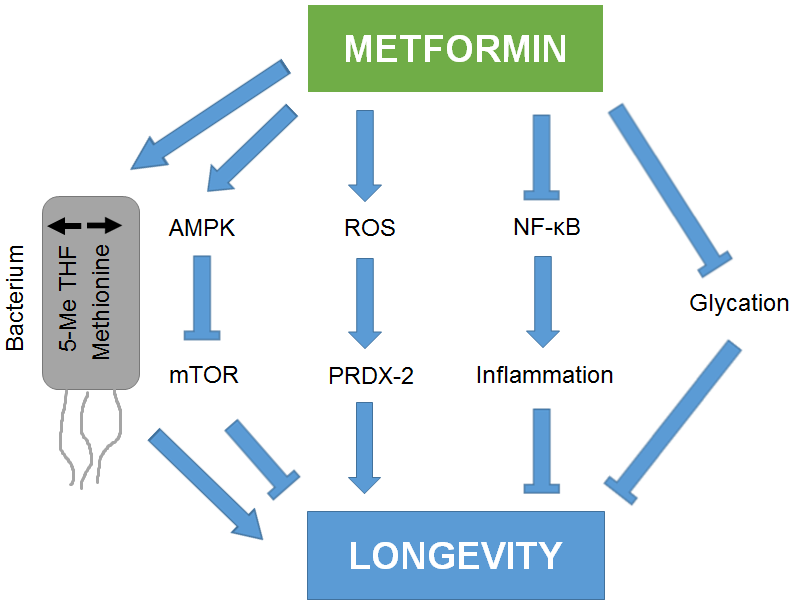
Figure 5 Some of the mechanisms through which metformin could promote longevity. The blunt-ended arrows indicate inhibition.
Metformin activates many pathways that have been linked to increased longevity including SIRT1 and FOXO and decreases pro-aging pathways like mTOR, insulin/IGF-1 signaling, and the proinflammatory transcription factor NF-κB. Metformin inhibits the formation of advanced glycation end products (AGEs) by scavenging the reactive intermediates (glyoxal and methylglyoxal) involved in AGE formation. Metformin also changes the metabolism of the microbiome leading to a decrease in dietary methionine content, which is known to extend lifespan in rodents. Metformin stimulates cell senescence in some experiments while reducing it in others. Interestingly, metformin may prevent the senescence-associated secretory phenotype (SASP) which is known to cause damage to surrounding tissues. Metformin reduced progerin expression and restored nuclear morphology in cells from Hutchinson-Gilford progeria patients. Metformin was also found to extend the lifespan of worms by inducing a mild stress (ROS production) in the mitochondria activating a protective response known as “mitohormesis”. However many studies find that metformin decreases ROS production, decreases oxidative damage, and upregulates the expression of antioxidant enzymes. Metformin may also lead to a slight decrease in body weight. However, the decrease observed in most studies in so small that it’s unlikely to have significant effects on health. The effects of metformin on autophagy, cell death, and DNA damage are discussed in the full text.
Side effects of metformin
Minor side effects
Metformin has several non-serious side effects such as gastrointestinal problems (diarrhea, flatulence, vomiting, upset stomach, abdominal bloating, anorexia, and nausea), taste disturbances including a metallic taste in the mouth, and dermatological problems (erythema, pruritus, and urticaria) (Product monograph: GlucophageⓇ, 2009).
Lactic acidosis
The most serious concern with biguanide therapy is the development of lactic acidosis. Lactic acidosis has a mortality rate of about 30-50%. The two other biguanides (phenformin and buformin) have been withdrawn because of the risk for lactic acidosis.
Salpeter and colleagues conducted a large meta-review of 347 studies and found no increased risk for lactic acidosis in metformin-treated patients compared to those on other diabetes medications. Furthermore blood lactate levels were not significantly different between both groups. The incidence of lactic acidosis is estimated at 5-9 cases per 100,000 patient years of metformin use. The lack of lactic acidosis cases in published trials probably reflects the fact that trials typically exclude patients at risk for lactic acidosis and that trial participants receive standard of care. Lactic acidosis is a risk especially in patients with contraindications for the use of metformin or in people who take an overdose.
Decrease in vitamin B12 and folate levels
Many studies have observed that metformin users have lower serum vitamin B12 levels compared to nonusers. Several studies also observed a decrease in serum folate levels in patients treated with metformin. However, not all studies observe a decline in folate levels.
In a meta-analysis of 29 studies with a total of over 8,000 patients it was demonstrated that metformin use was associated with lower serum vitamin B12 levels and a higher incidence of B12 deficiency.
Sadly many long-term users are never tested for vitamin B12 status. In fact current clinical guidelines do not make any recommendations on vitamin B12 testing or prevention in metformin users. In a recent study it was found that only 37% of long-term metformin users had their vitamin B12 status tested.
Decrease in testosterone levels
Multiple studies observe a decline in testosterone levels in women treated with metformin for either PCOS syndrome or breast cancer. There’s a surprising lack of male studies. One study found that two weeks of metformin treatment lead to a significant decline in total and free testosterone levels in normal males. Another study that combined metformin with a hypocaloric diet for three months found a decline in total testosterone levels in diabetic males and a decline in free testosterone in non-diabetic males.
Cognitive decline
Several studies report that metformin increases amyloid-beta production in cell culture. Leading many people to be concerned that metformin may promote Alzheimer’s disease. However there are two limitations to this conclusion. First, the dosages of metformin used in these studies greatly exceed those found in the brain after metformin administration. Secondly, when insulin was added to the cell culture metformin no longer increased amyloid-beta levels. In fact, amyloid-beta levels in cultured neurons exposed to metformin plus insulin were lower than in non-treated neurons. Insulin is present in the human brain.
Several human studies found that metformin use was associated with a higher risk for neurodegenerative diseases. Except in the Singapore Longitudinal Aging Study in which long term metformin use was actually associated with a reduced risk for cognitive decline.
One highly speculative explanation for the increased risk for Alzheimer’s disease found in diabetic patients is that diabetes patients develop neuronal insulin resistance. As discussed above metformin decreases amyloid-beta production in neurons in the presence of insulin while increasing it when insulin is absent. The insulin resistant brain state mimics the absence of insulin and in this condition metformin leads to an increase in amyloid-beta production and hence Alzheimer’s disease risk. In contrast, in the insulin sensitive (normal) state metformin might lower amyloid-beta levels and could hence maybe decrease Alzheimer’s disease risk. Though, I should stress again that this is speculation as no data exist on Alzheimer’s disease risk in non-diabetic metformin users.
Beta-cell function and apoptosis
Contradictory data exist on metformin's effect on pancreatic beta-cells. Some studies show that metformin causes beta-cell dysfunction and death while others find protective effects. However, all these studies have been conducted in cultured cells. To the best of my knowledge no data exist on metformin's effect on pancreatic beta-cell viability in whole organisms.
SUMMARY:
Based on current studies, the prospect of using metformin as part of a pro-longevity regimen merits further attention.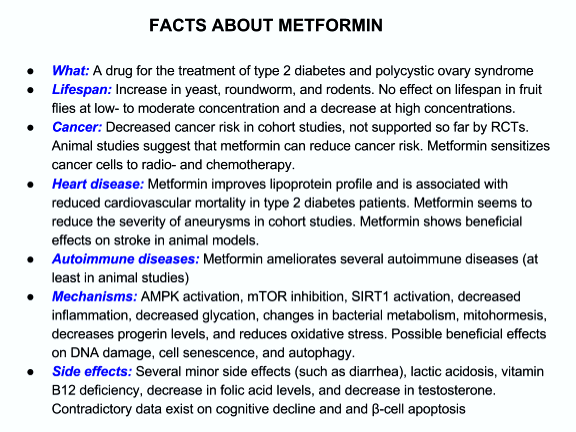 (click to enlarge)
(click to enlarge)
Summary slide: Metformin
NOTE: The information contained in this article is solely intended for information purposes and must not be held as substitute for professional medical or dietary advice. The provisos of the LongeCity user agreement apply. Neither the author nor LongeCity have financial interests in the sale or promotion of metformin.
CORRECTION: In the full text on page 32 in the first paragraph of the testosterone section the sentence "To the best of my knowledge no intervention study has tested the effect of metformin supplementation on lifespan." should say testosterone instead of metformin.
Extended version of this article:
Geroprotector review - Metformin.pdf (1.22MB)
downloads: 4097























{kind=link}
Thank you Sven for this nice article. I wonder if you develop more or point to what could potentially be a good dose for healthy humans? Sorry if I overlooked this in your summary.