


 LongeCity
LongeCityAdvocacy & Research for Unlimited Lifespans


I don't know where you can find that, but you can search for Trypsin (and even find beta-tryptase, I don't know the precise difference, you can find it trypsin relatively easy). Many are not familiar with this though this benefit lots of people, Trypsin/tryptase helps those with certain mutations, that on surface are helping longevity mechanisms, but taken as whole affecting the health of a person negatively. It helps those with mast-cell degranulation like disorders, allergies etc. It is an enzyme famous for protein digestion. I feel this is under-discussed topic and there should be a lot more conversation on it.

I've stopped sprint interval training (20-30 second sprints) and replaced with typical HIIT routine -- 10 min warmup, (2 min full out run, 3 min jog) x3 for a 25 minute workout twice a week. Results have been great, and I've, uh, recovered my VO2max (according to Apple Watch) from the drop I had when I replaced all runs with Sprint Intervals.
Wild-caught salmon, great! Looked at the study. I think you have it reversed. Pesco best for men, didn't reach statistical signficance for women.


Hey Cloomis, sorry I don't check in here very often but I'd love to respond even if late...
Interesting. Wasn't aware of those supplements affecting mitochondria. Do you do exercise targeted at mitochondria health as well?
What time do you do your intermittent fasting? It seems more beneficial if you start and stop earlier, when your insulin response for the day is the best.
HIIT/calisthenics routine?
Organic milk seems ok, but I would keep it under two cups a day. After that, it seems to increase all-cause mortality.
FIsh oil is good. I'm not familiar with most of the other supplements. Are you getting 150g of beans/day? They're the magic fruit for longevity as well. Also, 15g of nuts/seeds would help you as well.
I dont eat metformin anymore because i lost all my morning wood and aanything since i do excercise alot it decreasing my testosterone level what you guys think about this ?
I dont eat metformin anymore because i lost all my morning wood and aanything since i do excercise alot it decreasing my testosterone level what you guys think about this ?
Great job, Gordo. That takes a lot of dedication. I read your thread on CE as well. Excellent work.
You've thoroughly embraced CE. What's your opinion of saunas? I do two sets of 12 min. sauna followed by 5 min. cold bath (only 68 F, but that's what the local bath has) three times a week.
I see you've covered all the basics for plant food -- 1/2 oz. nuts, >5 oz. beans, veggies, fruits, etc. Have you considered adding fish? It's the only food category that adds longevity you don't have covered yet.
Probably don't need that inulin with how much plant-based food you're getting.
A Brazil nut a day? Shiver. I tried eating like three of those a week, and they made me light-headed. Ended up throwing away the pound I had bought.
You mention daily HIIT, which is solid. What do you do for low intensity physical activity and resistance training? Do you include sprint interval training or Tabata protocol or otherwise exceed 100% VO2max with your training?
Honestly, my comments would be minor tweaks. You have a solid routine, and have gone deep both on the plant-based diet and CE. Nice!

For users in the EU, meanwhile found also an exceptional German shop, some with even better options as listed in the OP:
2) D3: https://www.sunday.d...opfen-1000.html (many different versions available)
3) K2-mk7: https://www.sunday.d...-vegan-set.html (different versions, but no K2-mk4 or K1)
4) Omega-3: https://www.kraeuter...el-lemon-250-ml (different versions)
5) Vit C: https://shop-breinba...0/Products/1011 (up to 25kg)
6) Bs: https://www.sunday.d...2-mh3a-set.html (different versions)
8) A: https://www.sunday.d...ropfen-set.html (different versions)
10) E: https://www.sunday.d...formen-set.html (134mg tocopherols, of which ~20% non-alpha, and 100mg tocotrienols)
Didn't find real alternatives for:
1) Mg: Sunday.de does sell one including 7 forms at 100mg per capsule. Though with no disclosure of amounts as in propietary blends. This bulk shop might be an alternative for some: https://diacleanshop.../magnesium/?p=1 Also this expensive mineral water: https://en.wikipedia.org/wiki/Donat_Mg (1g per liter).
7) The multi-vitamin versions all suffers from too much iron, with the exception of this very incomplete only: https://www.sunday.d...-forte-set.html (also available low doses)
8) Other Tocopherols at high enough doses to balance the inhibition by alpha-tocopherol?
Full disclosure: No financial gains whatsoever through any of the presented options. Not even through referrals.
Edit re: 1) Mg: Sunday.de... amazing company, already within 1 month of writting this, they added high dose Mg-oxide (365 caps glass bottle), Mg-glycinate, Mg-malate, Mg-citrate and other forms to their sortiment. Some even as less expensive powdwers.
I'm not that worried about side effects, but I am worried that the possible beneficial effects of around 1 mg of lithium might be eliminated if it is allowed to accumulate too much.
Taurine might allow more lithium to accumulate in the body. Is this a cause for concern even with low-dose lithium? Would the lithium dose need to be adjusted?
As already repeatedly said, I would go by blood-testing to assure one's supplementation is in line with one's bio-chemical individuality. The only problem with blood-testing itself is, that normal reference ranges are usually established by assuming the middle 95% as normal. Therefore with decreasing intake of nutrients, normal reference ranges are of course trending downwards. Which I could already observe in the short time of a decade since doing blood-work.
Would be really telling to have access to historical nutrient reference ranges, like for example 50 years ago, or even ealier, when vitamins have been discovered.
Where did you get the notion 5-8:1 A:D was on a gram:gram basis? That is, source?
Frustrating basic vitamin ratios arent well established. This page talks about that ratio with some evidence, but its hardly conclusive. - Link
"Dr. Linday and her colleagues offer a suggestion: poultry studies suggest optimal A-to-D ratios between four and eight. Similarly, in her own studies showing that cod liver oil protects against upper respiratory tract infections, Linday supplied her patients with A-to-D ratios between five and eight.
They also point out that rat studies showing that vitamin A is toxic and antagonizes the effects of vitamin D used much higher ratios, ranging from 5,000 to 55,000!"
However I dont think the 5-8 ratio holds up if Weston Price's vitamin A daily intake is true. - Link
"The US Recommended Daily Allowance of vitamin A is currently 5,000 IU per day (and may possibly be lowered to 2500 IU per day). From the work of Weston Price, we can assume that the amount in indigenous diets was about 50,000 IU per day"
See also thehealthbeat.com where he gives a summary chart. - Link
"1. Native Eskimos: 5.4x calcium, 1.5x iron, 7.9x magnesium, 1.8x copper, 49x iodine, 10x vitamin A, 10x vitamin D
2. Indians of Northern Canada: 5.8x calcium, 5.8x phosphorus, 2.7x iron, 4.3x magnesium, 1.5x copper, 8.8x iodine,10x vitamin A, 10x vitamin D
3. High Mountain Swiss: 3.7x Calcium, 2.2x phosphorus, 2.5x magnesium, 3.1x iron, 10x vitamin A, 10x vitamin D
4. Gaelics in the Outer Hebrides: 2.1x calcium, 2.3x phosphorus, 1.3x magnesium, 1x iron, 10x vitamin A, 10x vitamin D
5. Aborigines of Austrailia: 4.6x calcium, 6.2x phosphorus, 17x magnesium, 50.6x iron, 10x vitamin A, 10x vitamin D
... there are more at the link"
I would welcome anymore thoughts on it.
So how are you doing with your stack? If I had been around at the time, I would have suggested dumping the pteorstilbene.
Moreover, that study was in aged horses , and the other studies I cited are consistent with nontrivial increased mTORC signaling with lysine supplementation - the real question, I imagine is whether the degree of activation via modest supplementation is clinically significant if one goal it to keep MTORC signaling on the low side.
Do you have any concern regarding stimulating mTORC1 from the periodic lysine you take at those doses?
While lysine does not invoke the same degree of stimulation on mTORC1 as, say, leucine, arginine, and glutamine, its contribution to mTORC1 stimulation above a threshold is nontrivial:
- https://www.ncbi.nlm...pubmed/24474444
- https://www.ncbi.nlm...pubmed/26366928
- https://www.ncbi.nlm...pubmed/30184226
Certainly, it has been argued that "While addition of lysine and/or methionine have been shown to increase phosphorylation of rpS6 and Akt in the muscle under certain conditions, these results are typically observed during periods of protein deficiency, or in in vitro studies" Source: https://onlinelibrar....1111/jpn.12992 ).
However your practice of CR - along with your practice of protein moderation - likely positions your insulin/igf-1 signaling (iis) pathway phenotypically with overlap with such a "low protein" model, given the substantial documented crosstalk between these nutrient sensing pathways.
Where did you get the notion 5-8:1 A:D was on a gram:gram basis? That is, source?
Ref: Excess Vitamin A Can Thwart Vitamin D
Osteoporosis is caused by a mismatch between vitamin A, D, and K2. The ideal A/D ratio wt/wt is about 5 to 1 which corresponds to an iu/iu ratio of 1 to 2.4 since 1 mg of vitamin A is 3,333 iu and 1 mg of vitamin D3 is 40,000 iu so 5 g to 1 g = (5)(3,333 iu)/40,000 iu = 1 to 2.4 iu/iu
Example: vitamin A retinol at 1,000 iu per day needs 2,400 iu per day of D3.
The "more is better" supplements are ridiculous--a quick look a Amazon show "vitamin A" in 5,000 to 25,000 iu capsules (likely mostly beta-carotene). A 25,000 iu dose of retinol would need to be balanced with 2.4 x 25,000 = 60,000 iu of D3. Perhaps you could take one 25,000 iu vitamin A (as retinol) per month and balance it with 2,000 iu of vitamin D3 daily.
Why not acarbose? As you noted "pretty promising results for acarbose as well." It well-established in diabetics management and without the same concern for immunosuppression/glucose tolerance/hypercholesterolemia, etc. as purported with rapamycin..
Side effects appear mostly limited to GI intolerance.
On that note, on allometric considerations:
A 0.02 kg mouse, on a "medium" dose of 1000 mg/kg (ppm) [ https://onlinelibrar...1111/acel.12898 ], the 20 mg dose comes to - for a 55 kg human - [ 0.75 exponent : http://clymer.alterv.../allometry.html ] about 7595 mg.
This is a lot more than 100 mg/meal ( or 300 mg/day ) maximum for acarbose. Is your concern that 100 mg / meal does not reproduce the effect?
OTOH, half life and metabolic rate considerations may not be an issue at all since the MOA is simply alpha glucosidase inhibition before it gets eliminated unchanged, Further, it appears the prescribed doses for diabetes blunt/ameliorate glucose spike to the extent that this is suspected ( along with microbiome alteration) a major posited mechanism of action: https://www.youtube....h?v=Jvj4Ba5E7GM
I'm still searching, but I doubt there is any research of A, D3 and K2 in combination with hard health outcomes yet.
Main reason why there are no nutrient-combination studies is, because the scientific method only tests 1 or 2 agents at a time, for limiting confounders. However, just came accross this surprising outcome of the TACT trial:
Effect of high-dose oral multivitamins and minerals in participants not treated with statins in the randomized Trial to Assess Chelation Therapy (TACT)
Intervention
Daily high-dose oral multivitamins and multiminerals (6 tablets, active or placebo).
Results
The primary end point occurred in 137 nonstatin participants (30%), of which 51 (23%) of 224 were in the active group and 86 (36%) of 236 were taking placebo (hazard ratio, 0.62; 95% confidence interval, 0.44-0.87; P = .006). Results in the key TACT secondary end point, a combination of cardiovascular mortality, stroke, or recurrent MI, was consistent in favoring the active vitamin group (hazard ratio, 0.46; 95% confidence interval, 0.28-0.75; P = .002). Multiple end point analyses were consistent with these results.
After 55 months there was a 9% absolute risk decrease in mortality compared to placebo!
Though for some nutrients they used a crazy dose (like 20mg of Manganese), the fat solubles were:
25,000 IU Vitamin A
100 IU Vitamin D3
400 IU Vitamin E
60 μg Vitamin K1
So the vitamin D and K amounts again almost not worth mentioning. Still such encouraging results, if for once they stop testing supplemented nutrients in isolation, but as they are actualy taken in combinations.
I'd be happy to discuss the pros and cons on the main forum (let's reserve this space for Michael's stack); in short possible cons in comparison to GS:
- greater lack of data for safety
- chondroitin is almost exclusively studied in combination with GS, which makes is hard to impossible to assess its effect
- lower bioavailability in trials
- several times higher price gram for gram
- unclear mechanism of action on cellular level
saying this: chondroitin might turn out to be a good idea. But the quality and scale of evidence is considerably below GS.
8. Deepen the spiritual connection
This is the greatest mistake in the treatment of diseases: that there are doctors for the body and physicians for the soul, where both can not be separated (Plato)
- experience spirituality
- a third kind of love
- the relationship between the physical and the spiritual
- it is important to exercise regularly
- it is important to calm the mind
Many of us are probably like me repulsed by superficial religious types, who only argue their religious superiority, but can't follow their proposed lifestyle themself. There are of course in every religion the opposite, not arguing but silently and contently following their paths.
In this respect, and just as my example - not do propose any superiority over any other religion or agnosticism - I found the old Pali text translations the closest I could identify with, where they talk about 10 fetters gradually and possibly to get free of:
Even beside other implications, for example just to become free of conceit would mean not considering oneself, better, worse or equal to any other. Just philosphically/poetically the only realistic stance for me possible, for not to perpetuate self-affliction in the one form or the other.
The proposed path through suffering/stress is straightforward:
Lawfulness of Progress, Anguttara Nikaya X, 1-2:
For one who is virtuous and endowed with virtue (Sila), there is no need for an act of will: 'May non-remorse arise in me!' It is a natural law, monks, that non-remorse (Kusala-sañña) will arise in one who is virtuous.
- For one free of remorse, there is no need for an act of will: 'May gladness arise in me!' It is a natural law that gladness (Pamojja) will arise in one who is free from remorse.
- For one who is glad at heart, there is no need for an act of will: 'May joy arise in me!' It is a natural law that joy (Piti) will arise in one who is glad at heart.
- For one who is joyful, there is no need for an act of will: 'May my body be serene!' It is a natural law that the body will be serene (Passaddhi) for one who is joyful.
- For one of serene body, there is no need for an act of will: 'May I feel happiness!' It is a natural law that one who is serene will feel happiness (Sukha).
- For one who is happy, there is no need for an act of will: 'May my mind be concentrated!' It is a natural law for one who is happy that the mind will be concentrated (Samma-samadhi).
- For one who is concentrated, there is no need for an act of will: 'May I know and see things as they really are!' It is a natural law for one a concentrated mind to know and see things as they really are (Ñanadassana).
- For one who knows and sees things as they really are, there is no need for an act of will: 'May I experience revulsion and dispassion!' It is a natural law for one who knows and sees things as they really are to experience revulsion and dispassion (Nibbida).
- For one who experiences revulsion and dispassion, there is no need for an act of will: 'May I realize the knowledge and vision of liberation!' It is a natural law for one who experiences revulsion and dispassion to realize the knowledge and vision of liberation (Nibbana).
...Thus, monks, the preceding qualities flow into the succeeding qualities; the succeeding qualities bring the preceding qualities to perfection, for going from the near to the far shore.
Or again in more detailed words:
Upanisa Sutta, Samyutta Nikaya XII:
'Just as, monks, when rain descends heavily upon some mountaintop, the water flows down along with the slope, and fills the clefts, gullies, and creeks; these being filled fill up the pools; these being filled fill up the ponds; these being filled fill up the streams; these being filled fill up the rivers; and the rivers being filled fill up the great ocean
- in the same way, monks, ignorance is the supporting condition for kamma formations, kamma formations are the supporting condition for consciousness, consciousness is the supporting condition for mentality-materiality, mentality- materiality is the supporting condition for the sixfold sense base, the sixfold sense base is the supporting condition for contact, contact is the supporting condition for feeling, feeling is the supporting condition for craving, craving is the supporting condition for clinging, clinging is the supporting condition for existence, existence is the supporting condition for birth, birth is the supporting condition for suffering,
- suffering is the supporting condition for faith, faith is the supporting condition for joy, joy is the supporting condition for rapture, rapture is the supporting condition for tranquility, tranquility is the supporting condition for happiness, happiness is the supporting condition for concentration, concentration is the supporting condition for the knowledge and vision of things as they really are, the knowledge and vision of things as they really are is the supporting condition for disenchantment, disenchantment is the supporting condition for dispassion, dispassion is the supporting condition for emancipation, and emancipation is the supporting condition for the knowledge of the destruction (of the cankers).'
But again, consider this just as example, how spirituality could be straigthforward experienced and integrated through an ethical and meditative practice. If one doesn't naturally inclines, these words could mean nothing more than gibberish. Follow your own inclination to free yourself from this schizophrenic reality split into body and mind, and by extension between physical and spiritual, me and others, holiness or sinning, etc. Choose a path you feel inclined.
.
Why not take glucosamine along with chondroitin? An analysis of the NHS and HPFS studies claims that glucosamine + chondroitin reduces CRC risk but not glucosamine without chondroitin.
Use of glucosamine and chondroitin supplements in relation to risk of colorectal cancer: Results from the Nurses' Health Study and Health Professionals follow-up study.
7. Allow social support
In poverty and misery, friends are the only refuge (Aristotle)
- experience love
- do not feel alone
- physical contact
The friend who appropriates, the friend who renders lip-service, the friend that flatters, the friend who brings ruin, these four as enemies the wise behold, avoid them from afar as paths of peril...
The friend who is a helpmate, the friend in happiness and woe, the friend who gives good counsel, the friend who sympathises too — these four as friends the wise behold and cherish them devotedly as does a mother her own child."— DN 31
6. Enhance positive emotions
The meaning of life is to be happy (Dalai Lama)
- what are positive emotions?
- what are the positive emotions in the body?
- happiness must be practiced daily
- but one does not have to be permanently happy
Think not lightly of good, saying, "It will not come to me." Drop by drop is the water pot filled. Likewise, the wise man, gathering it little by little, fills himself with good. - The Buddha
Or as in the also very old saying: "Gutta cavat lapidem" - Constant dripping hollows the stone.
as a further data-point for dose-depended effects, there is an in-vitro study, that demonstrates increasing downregulation of activation of mTor in a dose-dependent manner and upregulated AP in turn:
https://www.ncbi.nlm...les/PMC5983587/
That of course doesn't tell us, if the concentrations used are physiological - or if mTor is the major driver of autophagy in GS. At least one study conducted an experiment showing that GS still induces (increased) AP if mTor is silent:
https://www.scienced...025522?via=ihub
however, that increased AP is the major driver seems to become more and more clear:
https://www.jstage.j.../_html/-char/en
and as the mice-AP-paper demonstrates, GS is able to increase AP quite dramatically at physiologically achievable levels (much more than fasting by volume of AP-vesicles). In addition mitophagy (targeting damaged Mitos) seems to be up-regulated as well.
Therefore, given that both mice-paper (the life-span and the AP-paper) use doses that are closer to 6 g of oral intake per day; given that at least in the vital-data you can deduce a clear dose-dependent effect; and given the dose dependent inhibition of mTor by GS + especially the safety of GS.... could it be worth the risk, to take 3 g or 6 g per day? Or is it by Bayesian logic not also "risky" not to take more than 1,5 g - given the evidence so far?
5. Release oppressed emotions
Anger is an acid which can cause much greater damage to the vessel in which it is stored than to what it pours (Mark Twain)
- disease is blockade
- what are suppressed emotions?
- stress and cancer
- anxiety and cancer
- the waterfall solution
Through my extensive training of the past in mindfulness meditation and focusing therapy, I gladly already had many skills for inner-work with body, emotions and mind. However, whatever therapy, meditation or any other self-help method has in common, is the need of conducive circumstances: a safe place. Be it for allowing unskillful emotions, cultivating beneficial emotions, acknowledging help, spiritually reconnecting or finding a reason to live. All the remaining points up to the 9th on Kelly's list (of factors usually in place for remission in cancer-patients happening) really do need to a certain extent conducive circumstances.
The reality with chronic disease is very often the exact opposite. Living in a small city-flat not even knowing the names of one's neighbors, or being overwhelmed by the demands of modern day occupations, with little time for any respite, or having forgotten all this was meant for.
Not everyone is in the position to quit detrimental jobs or relationships yet. But what in my case really helped to create more space, was my yearly vacation for recuperation to a South Indian beach. Doesn't have to be expensive. For my mud-hut I pay about €1.50/day, a traditional meal with chai already under 1.-. The most expensive about my vacation is the running rent for my flat at home, not the flight.
Such a little yearly intervention for me (who already traveled India extensively in my youth, with absolutely no desire left having to see this and that, and thereby stress again) was conducive for so much all at once:
This is my main solar panel after 200 hrs/50 days in the South Indian sun this March:


I notice your productive attempt to punch some holes into my GS-obsession, so let's get started 
Obviously any translation from animal data is to some degree speculation. Allometric scaling for drugs tries to take account of different metabolic rates, but there is scant knowledge of differences in clearing of individual supplements by mice-detoxification mechanisms vs. humans - let alone if the supplement is even effective in humans. Nonetheless: as long as there is no better method available and lacking life-extension RCTs for humans, scaling the mice-data at the moment is the best life-extension data. Obviously useless if we wouldn't also have good reasons to assume, that the GS is effective in humans.
In respect to translating the mice data, the evidence is actually better than for Rapamycin. As you wrote before: total mortality for humans taking GS was quite notably reduced in a large-scale prospective cohort study in none-pathological people. We lack similar data for Rapa in humans... taking Rapa is based on the assumption, that the mTOR-connection is highly preserved and thus the life-extension effects seen in short lived animals (notwithstanding the question of not using allometric scaling for people taking it for LE).
Basis for the history of GS: Google
It's somewhat scattered over the internet, but you may start with one of those summarizing sources and their references
https://www.ncbi.nlm...les/PMC1120508/
https://www.ncbi.nlm...pubmed/15846645
https://www.thelance...0040-5/fulltext
long story short: based on some crude conclusions (glucosamine and chondroitine are part of cartilage... so taking it should improve cartilage) some veterinarians began first injecting it in animals; getting mixed results. A lack of good alternatives for osteoarthritis in humans and the compelling argument laid out before ("it's part of cartilage, so eating it improves cartilage") some pharma/supplement-companies began marketing different versions of GS for human consumption in the 90s. Despite no compelling results from studies, heavy publication bias and no good rationale for 1500 mg.
Yes. You are right. It's 3 g. Not 3 mg. It was a typo. I apologize for that and promise to be more careful in the future. I hope no one did assume, that I was jumping from 1500 mg to 3 mg.
Base: some inference based on the mice-autophagy paper:
https://www.ncbi.nlm...les/PMC3772083/
3 g per day was the mice equivalent administered to achieve the AP results, "beating" the human equivalent of a multi-day fast. This assumes that AP is a major driver of the effects of GS (which I personally find plausible, given GS apparent effect on cancer). The 3 g were injected though.
Better outcomes in humans: in some analysis of the vital data, participants reporting a higher intake of GS had (much) better cancer-results than low- and non-users:
https://www.ncbi.nlm...les/PMC3671752/
https://www.ncbi.nlm...les/PMC3175750/
As circumstantial evidence from the nurse-health-professional-study, people taking GS with normal BMI had much better results than overweight participants (after correcting for confounders):
https://www.ncbi.nlm...nihms799160.pdf
To be clear: if this would be Rapamycin I would be cautious about "overdosing" (aka going above the arbitrary 1,5g established by lack of evidence in the 90s). Side effects might occure not noted on lower dosis and U-shaped mortality curve is bound to set in at some point. But mega-dosing GS in rodents for up to a year lead to no notable side-effects in rodents. There doesn't appear an LD50 for rodents at very high doses either:
https://mafiadoc.com...bc5223bd8f.html
(note: this review actually reports LD50, while the original papers cited just state, that the LD50 must be somewhere above the maximum dose used in the studies).
And at least one-time mega-dosing GS in humans - that is injecting 30 g in one sitting - is well tolerated.
Now I'm not saying humans should inject 30 g of GS per day (which certainly requires a much higher oral intake, given the leveling-off of the bioavailability curve). But given how surprisingly harmless GS appears to be - even compared to metformin - I find it justified to get more in line of the mouse-lifespan-study. So more than 1,5 g/day.
Your take?
4. Take herbs and food supplements
The art of healing comes from nature and not from the physician (Paracelsus)
- help digestion: digestive enzymes, prebiotics and probiotics
- boost the immune system: e.g. Vitamin C, other vitamins (B12, D3, K2), fish oil, trace elements, certain edible fungi, aloe vera; and hormones (melatonin)
- detoxify the body:
- antimycotics (eg olive leaf extract, celery, nettle)
- antiparasitic substances (eg wormwood, yellow root, black nut husks)
- antibacterial and antiviral (eg garlic, oregano oil, Pau d'Arco)
- liver detoxification (eg milk spotted dwarf, dandelion root, sweet tooth root)
- supplements alone is not enough
The 60-thousand-dollar question about taking so many supplements (= what this all costs for 10 years; also the price of the vascular prosthesis declined), is always: Which part of it is essentially most effective? (- or belittled right away, since it allegedly could never been known anyway.)
The answer is of course always, that it depends on bio-chemical individuality. All the genetic susceptibilities, medical history and present conditions, deficiencies or overload, varying toxic exposures, diet and every other life-style factor, different metabolism, etc. In my case with difficulties with the heart, lung, liver, kidneys, spleen, androgens, thyroid, glucose metabolism, etc., - one could simply not hope ever to reverse the usually considered non-reversible main condition, if one didn't tackled even the slightest dysfunction of any body-system.
The best way for feedback I found in my case to be regular lab-work, after having educated myself about all the nutrients. Last year a new online-service: https://www.labtestanalyzer.com/ started, which after analyzing one's lab-work gives suggestions in respect having to get immediate medical attention, possibly helpful life-style and supplements interventions. All claims with scientific references right there to verify. Since this subscription service became too expensive after 1 year - with what I already learnt from it - in the end I entered all my average values for the last 10 years. The result: from 113 individual supplement suggestions all tailored to my lab-results, I already was taking 100 all these years (missing mainly probiotic strains). In the order of their importance by the number of individual lab-test, each supplement could affect beneficially in my case.
Vitamin D: Platelet Count, Eosinophils (Absolute), RBC, ALP, CRP, Hematocrit, Hemoglobin, Triglycerides, Insulin fasting, Albumin, Glucose fasting, HOMA-IR, Testosterone total, Triiodothyronine (T3) free, LDL-Cholesterol, Eosinophils (%), Thyroid Peroxidase (TPO) Abs, Lipoprotein (a), C-Peptide fasting, Glucose random
Zinc: Neutrophils (Absolute), RBC, ESR, CRP, Ferritin, Hematocrit, Hemoglobin, Triglycerides, Albumin, HOMA-IR, ACTH, Apolipoprotein B, Oxidized LDL
Vitamin C: Neutrophils (Absolute), RBC, ESR, CRP, Ferritin, Hematocrit, Hemoglobin, Triglycerides, Albumin, HOMA-IR, ACTH, Apolipoprotein B, Oxidized LDL
Green tea + EGCG: ALT, ESR, Transferrin Saturation, TIBC, Glucose fasting, HOMA-IR, VLDL-Cholesterol, TSH, ACTH, Glucose random, Transferrin
Fish Oil: ALP, ESR, CRP, Triglycerides, IgE, Albumin, VLDL-Cholesterol, LDL-Cholesterol, ACTH
Curcumin: BUN, ESR, Transferrin Saturation, TIBC, Insulin, Fasting, Albumin, Growth Hormone, Lipoprotein (a), Transferrin
Vitamin E: Neutrophils (Absolute), CRP, Hemoglobin, IgE, Albumin, Lipoprotein (a), Oxidized LDL, Apolipoprotein A1
Magnesium: Globulin, Reticulocytes, CRP, Triglycerides, Insulin fasting, Glucose fasting, Testosterone total, Glucose random
Vitamin B12: MCH, MCV, Platelet Count, RBC, Homocysteine, Vitamin C, Lipoprotein (a)
Selenium: WBC, CRP, Hematocrit, Hemoglobin, Albumin, Triiodothyronine (T3) free, Thyroid Peroxidase (TPO) Abs
Alpha-Lipoic Acid: ALT, Creatinine, Insulin fasting, Glucose fasting, VLDL-Cholesterol, Glucose random, Oxidized LDL
Lactobacillus plantarum (Probiotic): ALT, Homocysteine, Triglycerides, Bilirubin, Total, Insulin fasting, Glucose fasting, Glucose random
Calcium: CRP, Transferrin Saturation, TIBC, Testosterone total, Lipoprotein (a), C-Peptide fasting, Transferrin
5-MTHF: MCH, MCV, Platelet Count, RBC, Homocysteine, Albumin
Vitamin A: Eosinophils (Absolute), Ferritin, Hematocrit, Hemoglobin, Triiodothyronine (T3) free, Eosinophils (%)
Chromium: CRP, Insulin fasting, Glucose fasting, Glucose random, Resting Heart Rate, Apolipoprotein A1
Fenugreek: Triglycerides, Glucose fasting, HOMA-IR, VLDL-Cholesterol, Testosterone total, Glucose random
Garlic: Eosinophils (Absolute), CRP, Glucose fasting, Eosinophils (%), Glucose random
N-acetylcysteine (NAC): Neutrophils (Absolute), Homocysteine, Albumin, Triiodothyronine (T3) free, Oxidized LDL
Copper: RBC, Hematocrit, Hemoglobin, Vitamin C, Oxidized LDL
Bifidobacterium longum (Probiotic): ALT, CRP, Triglycerides, IgE, Glucose random
Resveratrol: Homocysteine, ESR, CRP, Apolipoprotein B, Oxidized LDL
Beta-carotene: Homocysteine, Hematocrit, Hemoglobin, Albumin, HOMA-IR
Ginseng: Creatinine, Triglycerides, Albumin, ACTH, Oxidized LDL
Grape seed extract: Transferrin Saturation, TIBC, HOMA-IR, Oxidized LDL, Transferrin
Cinnamon: Triglycerides, Insulin fasting, Glucose fasting, HOMA-IR, Glucose random
Omega 3-6-9: Monocytes (Absolute), Homocysteine, Apolipoprotein B, Resting Heart Rate
Ginkgo biloba: Eosinophils (Absolute), CRP, HOMA-IR, Eosinophils (%)
Sulforaphane/Broccoli sprouts: ALP, BUN, HOMA-IR, Oxidized LDL
Ginger: BUN, Triglycerides, HOMA-IR, VLDL-Cholesterol
Vitamin B3: CRP, Lipoprotein (a), Apolipoprotein B, Oxidized LDL
Red yeast rice extract: Triglycerides, Lipoprotein (a), Apolipoprotein B, Oxidized LDL
Beta glucans: Glucose, Fasting, Apolipoprotein B, Glucose, Random, Oxidized LDL
L-carnitine: TSH, Lipoprotein (a), Apolipoprotein B, Oxidized LDL
Boswellia serrata: Eosinophils (Absolute), ESR, Eosinophils (%)Zink: Uric Acid, Transferrin Saturation, Hemoglobin
Vitamin B6: RBC, Homocysteine, Lipoprotein (a)
Milk thistle: ALP, ALT, CRP
Ashwagandha: PaCO2, BUN, Testosterone total
Caffeine: PaO2, Bilirubin, Total, Growth Hormone
Lactobacillus rhamnosus (Probiotic): ALT, CRP, Glucose random
Pomegranate: BUN, CRP, Oxidized LDL
Cocoa: CRP, HOMA-IR, Oxidized LDL
Amla (Phyllanthus emblica): CRP, Triglycerides, VLDL-Cholesterol
Manganese: Transferrin Saturation, TIBC, Transferrin
Biotin (vitamin B7): Triglycerides, VLDL-Cholesterol, Lipoprotein (a)
Black Cumin Seed Oil (Nigella Sativa): Triglycerides, Bilirubin, Total, Thyroid Peroxidase (TPO) Abs
Vitamin B1: Albumin, Glucose fasting, Glucose random
Vitamin B9 (Folate): MCH, MCV
Rosemary: Eosinophils (Absolute), Eosinophils (%)
Spirulina: RBC, Creatinine
Lactobacillus fermentum (Probiotic): ALT, Glucose random
Lactobacillus delbrueckii (Probiotic): ALT, Glucose random
Bifidobacterium infantis (Probiotic): ALT, Glucose random
Flaxseed oil: BUN, HOMA-IR
Astaxanthin: CRP, Apolipoprotein B
Fructooligosaccharides (Prebiotic): CRP, Lipoprotein (a)
Quercetin: CRP, Oxidized LDLTongkat Ali: Hematocrit, Testosterone total
Soluble fiber: Albumin, Oxidized LDL
Pistachios: Glucose fasting, HOMA-IR
Arginine: VLDL-Cholesterol, Oxidized LDL
Phytosterols: Lipoprotein (a), Apolipoprotein B
Coenzyme Q10: Lipoprotein (a), Oxidized LDL
Inosine: Uric Acid
Glutathione: RBC
L-glutamine: RBC
TUDCA: ALP
Lavender: PaCO2
Cannabidiol (CBD): PaCO2
Melissa officinalis (lemon balm): PaCO2Betaine (TMG): Homocysteine
D-ribose: BUN
Suma root: BUN
Astragalus: Creatinine
Salvia miltiorrhiza (red sage): Creatinine
Nettle (Urtica dioica): Creatinine
Chamomile: Creatinine
Chitosan: Creatinine
Goji berries: ESR
Black tea: ESR
B-complex vitamins: Hematocrit
Blueberries: Triglycerides
Apple cider vinegar: Triglycerides
Apigenin: IgE
Luteolin: IgE
Yellow pea flour: Insulin fasting
Whey protein: Albumin
Vinegar: Glucose fasting
Vitamin K2: Vitamin D 25-Hydroxy
Shilajit: Testosterone total
Forskolin: Testosterone total
Tribulus terrestris: Testosterone free
DHEA: Testosterone free
Butea Superba: Testosterone free
Taurine: Triiodothyronine (T3) free
Iron: Triiodothyronine (T3) free
Kelp: TSH
Potassium: Aldosterone
Genistein: Thyroid Peroxidase (TPO) Abs
Phosphatidylserine: ACTH
Molybdenum: Ceruloplasmin
Soy Protein: SHBG
Boron: SHBG
Red clover (Trifolium pratense): Lipoprotein (a)
Mastic Gum: Lipoprotein (a)
Konjac glucomannan: Apolipoprotein B
Berberine: Apolipoprotein B
Bacillus coagulans (probiotic): Glucose random
Cranberry: Occult blood Urine
Nicotinamide: Apolipoprotein A1
EPA: Apolipoprotein A1
DHA: Apolipoprotein A1
Labtestanalyzer, due to sieving through the whole of the scientific literature manually for 1 year only, is still far from comprehensive or really reliable (always check their references), though they'll get there, one day.
By having to address virtually all dysfunctional body-systems, my targeted approach appears like the 'kitchen sink approach'. It isn't, and in most cases much less would have to be addressed.
In my case in retrospect, Linus Pauling's recommendations, along with K-vitamins, D3, CoQ10, omega-3, more magnesium, some aminos (taurine, carnitine, arginine..), most common plant-extracts (Garlic, Tea, Pomegranate..) , and a glucose-intolerance addressing diet - already improved my intermittent claudication limited walking distance from PAD the first 3 years from 10 minutes to 2 hours! When I stopped everything during that time for a 1-week water fast, intermittent claudication was temporarily back with vengeance. Only with a year long chronic bronchitis and COPD all that progress reversed it to half-hour again, and needed definitely a whole set of other interventions.
could you explain in a little more detail the rationale behind the 1500 mg per day dose?
It's the most commonly used dose in people using it as a joint-support supplement. So it ended up being the most common dose in cohort studies done in humans.
Yes ... exactly.
The mice-lifespan-study used the people-equivalent of 5-7 g per day.
I assume you're deriving this from the FDA HED calculation. Showing our math, in PMID 24714520, , the mice consumed ≈4 g of chow per day (Fig. 4a and Supplementary Fig. 2a,b), which contained 10 g/kg glucosamine), and weighed ≈33 g (Fig. 4d and Supplementary Fig. 2g–h). So that's [(.004 kg chow x {10,000 mg GLN/kg chow})/.033 kg body weight) ≈ 1212 mg GLN/kg mouse. Per HED, this is 98 mg/kg human = 6879 mg for a 70 kg human.
OTOH, per direct allometric scaling, it's even larger: 12502 mg!
It's important to remember that these methods of calculating human-equivalent doses are necessarily only very rough-and-ready: they can't account for any of the many ways that model organisms' metabolisms vary from ours — just the sheer metabolic rate. By contrast, 1500 mg is a human dose that's been wisely tested in clinical trials and used in the community for decades, that seems sufficient to have clinical effects and that the epidemiology suggests lowers mortality — and in this case, not likely because of healthy user bias, since people take GLS to relieve arthritis symptoms (and often other joint problems), and not because they're health-conscious.
On the other hand:
Also the side effects appear to be very limited compared to life-extension drugs such as metformin or rapamycin (human data).
I'd agree with you that glucosamine certainly seems safe, though I think we need to keep an eye (pun intended) on the possible IOP effect noted by Florian, above. More recently PMID 31104873 reported out "Effect of glucosamine sulfate on intraocular pressure in patients with knee osteoarthritis: A prospective randomized controlled trial," an open trial of 42 subjects finding "no differences in the IOPs between the groups (P>0.05) nor differences in baseline IOPs within each group compared with each follow-up visit (P>0.05)" between subjects receiving "1500mg of crystalline glucosamine sulfate once daily for 6 months [vs. controls]... at 6 weeks, 3 months, 6 months, and 9 months," which is a larger trial than the previous reports, but it's still small, was unblinded (ha ha), and was carried out in Thailand, where standards may not be as good. I'd also like to know the role of any sponsor in the trial, which isn't disclosed in the abstract and unfortunately I've not been able to acquire the full text.
Metformin is an extremely benign drug, although metformin is useless for life extension.
Certainly the side-effects of rapa are very serious and should be treated as such (though it bears remembering that the reported side-effects are from patients in very bad medical condition to begin with, and may not be as serious in otherwise-healthy aging people taking the same dose). OTOH, there is also a hell of a lot more data supporting its anti-aging effect than the single rodent study for GLS (and that, with no numbers, and a somewhat unclear, seemingly gender-specific, and unquantified effect on maximum lifespan).
Though it never had any particular basis even for joint support when established by rather less-scientific supplement companies/natural health remedies decades ago.
What is your basis for saying this?
The studies done in rodents indicate (if translatable to humans), that somewhere above 3 mg/day might lead to better life extension.
3 mg daily? I assume you mean 3 grams — yes? And where does this number come from?
In human cohort studies the most frequent intake/same intake for lower body mass - that is, a higher dose - generally lead to better outcomes.
What is your evidence for this?
It could be argued, that people can't get the mice-benefits of rapamycin, as they are unable to sustain the side effects of mice-equivalent administration.
Certainly it seems likely that the effective dose for life extension with rapamycin will be lot higher than the 5 mg once a week being widely adopted on the basis of Alan Green's say-so. I see you agree, albeit that I think you may overstate your case somewhat. But we don't really know if the side-effects are tolerable as there are so few cases of people even trying.
On that on glucosamine, have you found any supplements in the sulfate formulation that are 1500 mg per tablet?
No, but I haven't looked: I avoid tablets in favor of capsules where possible because they're so often screwed up (turned into little insoluble pebbles), and 1000 mg tablets would likely be difficult to swallow.
My error on the ubiquinol: I take 50 mg. This is probably leftover typing from when I was taking 10 mg of ubiquinone ("regular" CoQ10).
3. Follow your own intuition
In vital matters, the decision should come from the unconscious, somewhere from within (Sigmund Freud)
- listen to body signals
- activate the intuition
- find the right change
Again, a bid difficult for those of us less intuitive to even understand what this could mean. In my case was always attracted to explore beyond linear reasoning, and had long trainings in body-signal oriented focusing and mindfulness meditation practice.
With the later more intended to train in 'letting go', also the '..it's as if my life depended on it..' came from such a different place. Total alien to how I usually organize my life.
On that on glucosamine, have you found any supplements in the sulfate formulation that are 1500 mg per tablet?
I have only found up to 1000 mg per tablet in the glucosamine sulfate form ( pure encapsulations). If you know a brand, please share.
@ Michael: I find your general approach and evidence based regimen rather useful. Given the amount of expertise you put into your supplement regimen just one question. As a little side-obsession on my part I have read a little bit of the Glucosamine literature. Therefore, could you explain in a little more detail the rationale behind the 1500 mg per day dose?
It's the most commonly used dose in people using it as a joint-support supplement. So it ended up being the most common dose in cohort studies done in humans. Though it never had any particular basis even for joint support when established by rather less-scientific supplement companies/natural health remedies decades ago.
The studies done in rodents indicate (if translatable to humans), that somewhere above 3 mg/day might lead to better life extension. The mice-lifespan-study used the people-equivalent of 5-7 g per day. In human cohort studies the most frequent intake/same intake for lower body mass - that is, a higher dose - generally lead to better outcomes. Also the side effects appear to be very limited compared to life-extension drugs such as metformin or rapamycin (human data).
It could be argued, that people can't get the mice-benefits of rapamycin, as they are unable to sustain the side effects of mice-equivalent administration. The same can't be said for glucosamine. So.... why do you see 1,5 g as more justified over 3 g or even 6 g ?
2. Take control of health
Action is the basic key to success (Pablo Picasso)
- actively participate
- be prepared for change
- resolve resistance
I guess point 2 is already a big stumbling block for most patients. My GP tells me that I'm his only of his patients asking for particular lab-tests, and taking copies of all. Additionally, for most conventional docs met, that alone is already offensive, that as a patient one has to be prepared to receive a lot of abuse.
My worst example, asked the cardiologist who pushed an invasive vascular prosthesis on me: What would be the risks compared for example to a simple balloon angioplasty? (the later being in use for the longest time). On which the only answer was, that balloon angioplasty wouldn't be performed in our country anymore. To get at least some response about risks and being enabled for an informed decision, I dared to challenge: If this preference for vascular prosthesis could in any way be influenced by its higher financial profit? On which this cardiologist ended the conversation. With the remark that he actually isn't a cardiologist, but just stepped in for an other.
Half a year later I tried again, in the hope the first cardiologist not being on duty. In vain, I met the same again. Now he refused any conversation with the excuse, that he already explained everything in detail at the first occasion. My question: Why then the last time he denied being a cardiologist? - his face turned red - and said: I actually would suffer from personality disorder, and for that should better show up at the psychiatric department! - However, I still insisted to be informed of any risk to the pushed procedure, and had to wait a whole 4 hour for finally an other cardiologist showing up. Though staying a bit more professional, the second cardiologist could only inform me of acute risks during the procedure (1 in a 100; for which he had to phone a colleague to get the information).
Really both showing so much ignorance or lack of integrity, which alone would be enough reason not to ever have such an invasive procedure with any of them.
On the German wikipedia I finally found the simple answers, and I even suggested in my own words during the consultations with the cardiologists, for being enabled for an informed decision:
The most frequent complications after the use of vascular prostheses are blockage (occlusion) due to excessive tissue formation in the neointima region (hyperplasia) or due to detachment of parts of the pseudointima, infections of the implant, problems with the material structure, as well as the development of aneurysms and pseudoaneurysms in the anastomosis region.
Five to ten years after implantation, around 90 percent of prostheses still function in the aorta area and the adjacent vessels, while prostheses with a diameter of less than six to eight millimeters have a success rate of less than 50 percent after five years. In general, the higher the flow resistance in the implant area, the lower the prospects for short-term and long-term function.
(translated with DeepL)
A very good resource for someone not used to verify primary research yet, is http://www.thennt.com. The risk/benefit ratio found there for the prescriptions/intervention intended for me till my deathbed (docs never advised, even denied and ridiculed):
Statins Given for 5 Years for Heart Disease Prevention (With Known Heart Disease)
83 for mortality
In Summary, for those who took the statin for 5 years:
Benefits in NNT
- 1 in 83 were helped (life saved)
- 1 in 39 were helped (preventing non-fatal heart attack)
- 1 in 125 were helped (preventing stroke)
Harms in NNH
- 1 in 100 were harmed (develop diabetes*)
- 1 in 10 were harmed (muscle damage)
*The development of diabetes is one such unanticipated harm found in a recent large study and it seems likely therefore that this applies to the data above, although this is a best guess.
Aspirin to Prevent Cardiovascular Disease in Patients with Known Heart Disease or Strokes
333 for mortality
In Summary, for those who took the aspirin:
Benefits in NNT
- 1 in 50 were helped (cardiovascular problem prevented)
- 1 in 333 were helped (prevented death)
- 1 in 77 were helped (prevented non-fatal heart attack)
- 1 in 200 were helped (prevented non-fatal stroke)
Harms in NNH
- 1 in 400 were harmed (major bleeding event*)
*Required hospital admission and transfusion
Blood Pressure Medicines for Five Years to Prevent Death, Heart Attacks, and Strokes
125 for mortality
In Summary, for those who took anti-hypertensives:
Benefits in NNT
- 1 in 125 were helped (prevented death)
- 1 in 67 were helped (prevented stroke)
- 1 in 100 were helped (prevented heart attack*)
Harms in NNH
- 1 in 10 were harmed (medication side effects, stopping the drug)
*fatal and non-fatal myocardial infarction and sudden or rapid cardiac death
Clopidogrel Added to Aspirin to Prevent a Second Heart Attack Or Stroke
None for mortality
In Summary, for those who took the clopidogrel:
Benefits in NNT
- None were helped (cardiovascular problem prevented)
Harms in NNT
- 1 in 167 were harmed (major bleeding event*)
Coronary Stenting for Non-Acute Coronary Disease Compared to Medical Therapy
None for mortality
In Summary, for those who received the stenting:
Benefits in NNT
- None were helped (life saved, heart attack prevented, symptoms reduced)
Harms in NNH
- 1 in 50 were harmed (complications such as bleeding, stroke, kidney damage)
For me enduring such resistance and even adverseness, as well as being prepared for lifestyle changes, wasn't an issue - it's as if my life depended on it.
This study sums the state of cardiology up:
JAMA. 2019 Mar 19;321(11):1069-1080. doi: 10.1001/jama.2019.1122.
Levels of Evidence Supporting American College of Cardiology/American Heart Association and European Society of Cardiology Guidelines, 2008-2018.Abstract
Importance:Clinical decisions are ideally based on evidence generated from multiple randomized controlled trials (RCTs) evaluating clinical outcomes, but historically, few clinical guideline recommendations have been based entirely on this type of evidence.
Objective:
To determine the class and level of evidence (LOE) supporting current major cardiovascular society guideline recommendations, and changes in LOE over time.
Data Sources:
Current American College of Cardiology/American Heart Association (ACC/AHA) and European Society of Cardiology (ESC) clinical guideline documents (2008-2018), as identified on cardiovascular society websites, and immediate predecessors to these guideline documents (1999-2014), as referenced in current guideline documents.
Study Selection:
Comprehensive guideline documents including recommendations organized by class and LOE.
Data Extraction and Synthesis:
The number of recommendations and the distribution of LOE (A [supported by data from multiple RCTs or a single, large RCT], B [supported by data from observational studies or a single RCT], and C [supported by expert opinion only]) were determined for each guideline document.
Main Outcomes and Measures:
The proportion of guideline recommendations supported by evidence from multiple RCTs (LOE A).
Results:
Across 26 current ACC/AHA guidelines (2930 recommendations; median, 121 recommendations per guideline [25th-75th percentiles, 76-155]), 248 recommendations (8.5%) were classified as LOE A, 1465 (50.0%) as LOE B, and 1217 (41.5%) as LOE C. The median proportion of LOE A recommendations was 7.9% (25th-75th percentiles, 0.9%-15.2%). Across 25 current ESC guideline documents (3399 recommendations; median, 130 recommendations per guideline [25th-75th percentiles, 111-154]), 484 recommendations (14.2%) were classified as LOE A, 1053 (31.0%) as LOE B, and 1862 (54.8%) as LOE C. When comparing current guidelines with prior versions, the proportion of recommendations that were LOE A did not increase in either ACC/AHA (median, 9.0% [current] vs 11.7% [prior]) or ESC guidelines (median, 15.1% [current] vs 17.6% [prior]).
Conclusions and Relevance:
Among recommendations in major cardiovascular society guidelines, only a small percentage were supported by evidence from multiple RCTs or a single, large RCT. This pattern does not appear to have meaningfully improved from 2008 to 2018.
1. Radically change the diet
Let your food be your medicine, and medicine your food (Hippocrates)
- avoid sugar, meat, dairy products and processed foods
- eat lots of fruits and vegetables
- limit to organic food
- drink only filtered water
Some of the cancer patients interviewed by Kelly did actually the opposite, and added meat back in. Same in my case, having been low fat vegetarian (only cheeses) for more than 30 years since age 10, I added loads of healthy fats (~70% of calories), daily eggs and weekly fish short after my PAD diagnosis back in, much later some occasional meat. Due to low budget, I limited to organic food where it counts though (like the dirty dozens veggies and fruits, as well as all animal based food).
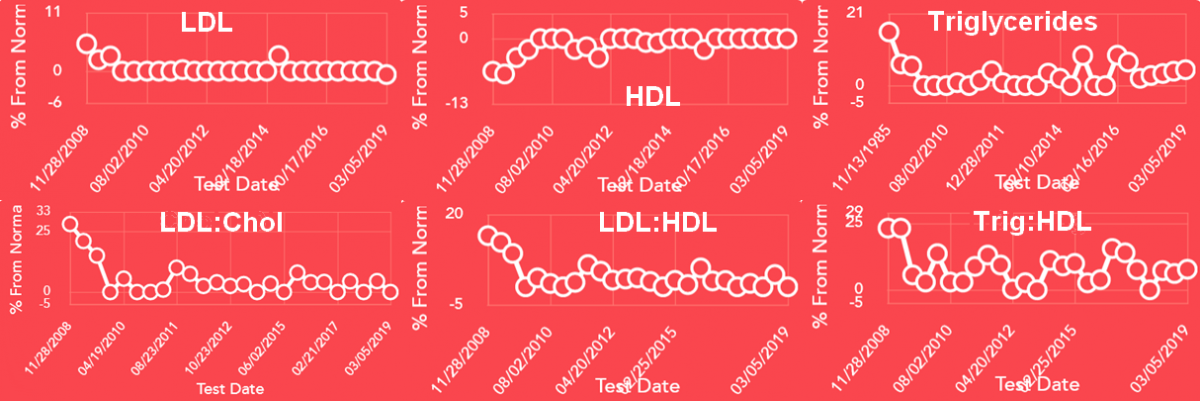
The effects of such a diet change to my basic lipo-proteins during the last 10 years:
One framework to explain such differences in bio-chemical individuality would be different autonomous-nervous system metabolic types, used for example by the late pancreatic cancer doc Nickolas Gonzales (the following notes taken from an interview):
Dominant sympathetic types: Typ ‘A’ personalities, disciplined; mostly solid cancers; do good on much plant based foods: fruits, vegies, seeds, grains, nuts, plant based oils: hemp, flax; Vitamin B1, B2, B3, 8:1 ratio magnesium to calcium, high vitamin C & D; but not on much meat protein, no b12, no choline, no B5, no zinc, no selenium, no fish oil. Yes to beta Carotene, chromium, folic acid, riboflavin, thiamin,& niacin
Parasympathetic: types are rather creative with unconventional ‘formal’ education; mostly blood-based cancers; do good on lots of meat and a ketogenic diet, saturated fats, fats from fish oils, Calcium 10-15 ratio to magnesium (high magnesium causes depression), Vitamin B12, B5, Choline; not as good on grains or seed. Need zinc & selenium, not good with other large Vitamin B doses.
Mixed or balanced types: suffer rather from allergies and fatigue.
One fact I did come across at the beginning of my health journey which really piqued my interest is, that some traditional diets still contain about a 100 different plants per year, each containing again up to 100 phyto-nutrients, often most not identified yet. Before the agricultural period humans consumed even up to 200 different plants per year. One impact of such a varied diet seems to become apparent with the micro-biome research:
http://ucsdnews.ucsd...ats-in-your-gut
Big data dump from the world’s largest citizen science microbiome project reveals how factors such as diet, antibiotics and mental health status can influence the microbial and molecular makeup of your gut
Emerging trends
All of the data collected by the American Gut Project are publicly available, without participants’ identifying information. This open access approach allows researchers around the world to mine the data for meaningful associations between factors such as diet, exercise, lifestyle, microbial makeup and health. Here are a few observations that have emerged so far:
Diet. The number of plant types in a person’s diet plays a role in the diversity of his or her gut microbiome—the number of different types of bacteria living there. No matter the diet they prescribed to (vegetarian, vegan, etc.), participants who ate more than 30 different plant types per week (41 people) had gut microbiomes that were more diverse than those who ate 10 or fewer types of plants per week (44 people). The gut samples of these two groups also differed in the types of molecules present.
Antibiotics. The gut microbiomes of American Gut Project participants who reported that they took antibiotics in the past month (139 people) were, as predicted, less diverse than people who reported that they had not taken antibiotics in the last year (117 people). But, paradoxically, people who had taken antibiotics recently had significantly greater diversity in the types of chemicals in their gut samples than those who had not taken antibiotics in the past year.
The participants who ate more than 30 plants per week also had fewer antibiotic resistance genes in their gut microbiomes than people who ate 10 or fewer plants. In other words, the bacteria living in the guts of the plant-lovers had fewer genes that encode the molecular pumps that help the bacteria avoid antibiotics. This study didn’t address why this might be the case, but the researchers think it could be because people who eat fewer plants may instead be eating more meat from antibiotic-treated animals or processed foods with antibiotics added as a preservative, which may favor the survival of antibiotic-resistant bacteria...
In my case counted up to 70 different plants eaten a year (and sure forgot some):
And my only ubiome-result from 2 years ago seems to confirm: http://tinyurl.com/mircrobiome. In that my microbiome was more diverse than 93% of all tested at that time.
Since it would probably take me days to enter my actual regimen with up to 500 ingredients (dietary and supplemental), something much more accurate: All that as it changed over the 8 years - click the below link for the detailed regimen -
https://docs.google....#gid=1308885060
That high number only came about by counting each macro- and micro-nutrient, phyto-chemical, and their respective sources noted in my spreadsheet. Without such at times multiple count it's about half. And actually taken also about 250 individual supplements (caps or pills) or powders (spices, herbs..). In about a half/half ratio. Therefore really not that far off in filling in gaps and replicating a pre-agricultural really varied diet.
2 years later its time for an update:
No more postexcertional malaise since! Hallelujah :-)
Though I kept very strict at pacing, at occasions I couldn't - or with much less sleeping hours - it still caused no real PEM anymore.
Also my maximal carotid intima-media thickness (CIMT) for the first time last year remarkably regressed. Normal would be below 0.9 mm.
In below table I added max. pain-free walking distance (PFWD; in kms at about 4/hr), Erythrocyte sedimentation rate (ESR), C-reactive Protein (CRP), and Ankle Brachial Index (ABI; normal ≥9). Vitamin D intake (mcg), serum level (25-OH-D), whole-body sun-exposure (hrs/year), and total testosterone (TT) for their very strong correlation. The very high inflammation in '06, 2 years before the PAD diagnosis, was caused by a Myopericarditis.
year: PFWD ESR CRP ABI mcg hrs 25-D TT CIMT 2006: - 74 96 - - - - - - - - - - - - - - - - 2008: 0.3 5 - 0.7 - - - - - 2009: 1 8 1.6 - 50 - - - - 2010: 4 15.5 3.4 - 160 60 63 399 - 2011: 6 4 2.4 0.5 240 60 43 220 - 2012: 3 - 5.2 0.8 300 60 62 262 1.3 mm 2013: 3.5 68.5 3.7 - 200 220 84 320 - 2014: 5 9 4.8 0.7 190 220 50 340 1.9 mm 2015: 8 11.5 2.5 - 210 220 78 351 - 2016: 9 8 1.1 0.7 170 240 72 468 1.8 mm 2017: 9 18 1.7 - 220 340 101 631 - 2018: - 32 5.1 0.9 160 340 93 681 1.0 mm 2019: - 18.5 2 - 190 340 85 368 -
Seems the high inflammation with the year long chronic bronchitis in '12 progressed CIMT quite some further (a 20% yearly increase), and only around the time I lost my walking-disability it started to regress.
(note: above are yearly averages if more than 1 data-point was available, for example highest hsCRP in '12 was 7.6 mg/l, following ESR in '13 actually 130 mm/hr; highest 25(OH)D 135 ng/ml, lowest total testosterone 187 ng/dl)
Regarding "the timing of glycine (either for sleep or life extension) and lysine are specific to their use, and are to maintain continuous serum exposure, not to increase bioavailability AUC," possibly for lysine, and certainly for glycine ( which you are not presently taking), I am curious how the pharmacokinetics and pharmacodynamics might be influenced by meals.
That is, while spacing out the glycine regularly may keep the serum exposure more uniform, could some benefits of glycine supplementation be in relative to that of other serum amino acid levels at the time of intake? If so, this would be influenced by intake relative to meals-
To be concrete, if I take all my glycine during a single daily meal, I would certainly would absorb less glycine by competitive inhibition via other dietary amino acids, however I can presumably compensate for this by increasing the glycine dose taken with that daily meal. On the other hand, the glycine that I do take that meal may have the advantage of contributing to less absorption of methionine and/or the nutrient sensing sequela of said methionine, by maintaining higher hepatic glycine levels.
Hi Michael,
Your comments were again valuable.
Please keep any corrections coming - though I know the difference ( autocorrect at work?), and noticed the systematic error in the posting, I could not edit it out with attempts to edit unsaved. Hence the two posts back-to-back. Personally my pet peeve - is loose vs lose!
So you type references by hand every time, in full, numbers and all, or is there a part of PubMed or your favorite search engine where the full citation is appropriately formatted in full? For example if you are citing https://www.ncbi.nlm...les/PMC5715805/ , do you click on "Citation" on the upper right and then select "AMA Format" or do you have another method? I have published lengthy manuscripts offline using citation managers embedded within my word processor, but have not thus far for web-forum posts which I admittedly type on the fly bypassing the word processor. Perhaps I should reconsider my practices for quality control considerations.
I agree with your comments regarding Attia, and thought the link illustrated it well. I do enjoy them both, though Patrick admittedly seems at time prone to over-excitement and consequently asymmetric presentation and endorsement of a particular pet subject ( say NRF2 enhancers, broccoli sprouts, and Sauna therapy). It would be great to have more of a synthesis with contradictory findings or something akin to AUB's "contrary/null findings" https://shockcenter.uab.edu/ To her credit though she does a much better job than 99.9% of the healthspan sphere trying to present data in perspective, and they both also share a higher degree of transparency, minimization of conflict of interest, and interest in scientific integrity which is sadly uncommon in this space.
I share many Attia's "obsessions" and philosophy of "strong convictions, loosely held," esp. "loosely held," and like Attia I find that as my absolute knowledge in longevity science expands my perception of my relative knowledge diminishes precipitously  This is humbling but motivates me to dig deeper.
This is humbling but motivates me to dig deeper.
At this point, my next step is evaluating alternative regiments and possible additions.
You mean "regimen," not "regiment" . I am amazed by how many people make this error: there's a whole regiment of them on Longecity alone.
For your glycine ( I know you are not using this one), lysine, and taurine, would you feel comfortable with taking 1000+ mg at a time rather than 500 divided from a safety and tolerance perspective? As you alluded to, you divide primarily for either greater absorption, or to spread out the serum levels so that it can be more biovailable more of the time. In drawing my own health optimization versus convenience regiment I am entertaining taking daily, in the 1000-2000 mg range recognizing this may be less effective than your carefully cultivated regimen; are there liabilities I may be overseeing besides and accepting the efficacy vs convenience tradeoff?
It might be fine with taurine, but the timing of glycine (either for sleep or life extension) and lysine are specific to their use, and are to maintain continuous serum exposure, not to increase bioavailability AUC: see the discussion in the post.
On the subject of possible additions, in a non-diabetic without hyperlipidemia, do you see any benefit for berberine.
I've seen far too little long-term human or animal data on either safety or efficacy. I'm not at all convinced by the limited animal evidence that it even is a PCSK9 inhibitor, even in rodents — and if it is, if the effect is durable, since if it happens at all it happens at the transcription regulatory level, which could very well gradually fade due to feedback systems. Moreover, lat time I looked, all the human trials with LDL-C outcomes that have been done in nondiabetics (which is the relevant study design for a PCSK9 inhibitor) have not only been small and short-term, but have used combinations with red yeast rice and often many other ingredients, so one doesn't know what if any contribution the berberine is making — or, again, if it's durable.
And would you hesitate to take both a metformin and PCSK9 together or might the double AMPK mechanism of action be beneficially synergistic without too much concern about deleterious synergy?
I focus on empirical outcomes, not mechanisms, and I'm not impressed that AMPK is a good target to focus on even granted that; nor am I convinced that it's a particularly important mediator for either metformin or berberine. And if it were, and we were to wallow in mechanistic speculation on the question: usually when you get an effect of 2 different agents that work through the same mechanism, it's more likely that you get a sub-additive effect than a synergistic or even additive one, unless one of them comes at it both potently and upstream rather than directly: there's only so far one can push these things holding genetics and lifestyle constant.
I noticed that you cite your references. What citation manager do you use?
I don't use one.
Also, since I mentioned him, would be interested in your take on Dr. Attia. I don't know much about him but he seems to be increasingly positioning himself in the translational longevity space. He and Dr. Rhonda Patrick seem to be brining to the mainstream some ideas formerly restricted more narrowly to Longecity and the broader LE grassroots and research communities.
I'm impressed by Dr. Attia — not so much for his knowledge (which is extensive) or his views (with which I not infrequently disagree), but for his self-enforced intellectual humility (he admits that this is effort for him, his default tendency being toward overzealous confidence in his views), his data-driven approach, and agnosticism. I get thie impression that he has evolved on these issues quite significantly as a result of his experiences at NuSi and the drivers of his departure from same. He has his frameworks and preferred hypotheses but is decidedly nondogmatic about them, and doesn't try to force the data on an individual patient into them when they clearly don't fit (viz. his arguments with people who insist that they can ignore a sky-high LDL-P so long as it's the result of a ketogenic diet, their CRP is low, and they don't have any coronary calcium). He also has great guests on his podcast, and can glean a lot of value from what would seem to be an unpromising guest.
By contrast, while Patrick also often has good guests, she has the unfortunate tendency of stating preliminary hypotheses as facts, and equally of a kind of intellectual passive-aggressiveness; she also fails to take in the key heuristic captured in the Attiaism "That's a fact, but is it a reason?" This last point is well illustrated in the lengthy exchange that Attia and Patrick have in her podcast "Peter Attia, M.D. on Macronutrient Thresholds for Longevity" etc, starting around 25:33 (in the transcript, beginning at "I like to think about it at the level of the gut" etc).
Hmmm, I can't seem to edit my post successfully with it saving the changes. Wanted to add this interesting summary regarding its positioning in nutrient sensing pathways ( see: https://www.ncbi.nlm...les/PMC5839379/ )- I know you are not generally very convinced nor am I without strong long-term observational data with quality trials at leaset in model organisms if not people..... however, if ( a big if depending on your response) it is deemed low risk as a supplement dosing, might thislower the threshold to supplement with its interesting mechanistic and some albeit not ideal supportive clinical data at this point?
Also, since I mentioned him, would be interested in your take on Dr. Attia. I don't know much about him but he seems to be increasingly positioning himself in the translational longevity space. He and Dr. Rhonda Patrick seem to be brining to the mainstream some ideas formerly restricted more narrowly to Longecity and the broader LE grassroots and research communities.
That's a great list. Some are straightforward such as UL / USP / NSF certification. Others compel investigation, such as sharing third-party certificates, and yet others are have subjective as well as objective information such as responsiveness to inquiries, transparency, etc. This last category is easiest to assess based on past experiences. Do you feel comfortable naming the brands you felt passed the last and presumably also other criteria? Reliability and quality may be a moving target, but starting with those "so far, so good" companies would not be a bad start.
I have "graduated" assessing you full list and have incorporated several new supplements thanks to your post with only modest departures. At this point, my next step is evaluating alternative regiments and possible additions.
For your glycine ( I know you are not using this one), lysine, and taurine, would you feel comfortable with taking 1000+ mg at a time rather than 500 divided from a safety and tolerance perspective? As you alluded to, you divide primarily for either greater absorption, or to spread out the serum levels so that it can be more biovailable more of the time. In drawing my own health optimization versus convenience regiment I am entertaining taking daily, in the 1000-2000 mg range recognizing this may be less effective than your carefully cultivated regimen; are there liabilities I may be overseeing besides and accepting the efficacy vs convenience tradeoff?
On the subject of possible additions, in a non-diabetic without hyperlipidemia, do you see any benefit for berberine. I read your comments about metformin above and realize it has never as unitherapy yielded good evidence for life-extension ( indeed, quite the oppososite). However despite the overlap with AMPK mechanism of action with metformin, berberine may also act as a PCSK9 inhibitor. There is an additional question of bioavailability, though it least some formulations are purported to have greater nonavailability [ https://onlinelibrar...0.1002/ptr.6282 ], and berberine has additional potential albeit theoretical benefits including as Darryl recently pointed out in another thread systemic rather than strictly hepatic circulation as is the case for metformin. As for the PCSK9 inhibition, anecdotally Peter Attia in an interview recently related his clinical experience that high PCSK9 producers tend to see their LDL go down by about 20% when used for this purpose - Incidentally, what is your take on Attia in the longevity space? IAC, aside from PCSK9, berberine influences nutrient sensing in other potentially beneficial ways [ https://www.ncbi.nlm...les/PMC5839379/ ], which if low-risk may perhaps justify a lower threshold to supplement despite less-than-convincing outcomes assessments thus far.
You have not stated your lipid profile, but even on the last point alone, why not lower your LDL further, the the evidence from PCSK9 inhibitors (e.g., the from the FOURIER trial), with evidence getting the LDL is low as <=30 potentially yielded benefit. While metformin has its own inconveniences in and intolerances ( lower the anerobic lactic acid threshold with possible fatigue and GI intolerance), it seems at first glance PCSK9 may be a lower risk addition to your regimen. Or are your concerns over genotoxicity or other matters greater than that expressed by others at a clinical dose of say 1000 mg twice daily - your thoughts?
And would you hesitate to take both a metformin and PCSK9 together or might the double AMPK mechanism of action be beneficially synergistic without too much concern about deleterious synergy?
Finally, if applicable, if you did select a berberine supplement at some point, which formulation and brand would you trust most for fidelity and bypassing the first pass effect?.
Footnote: off-topic but germane to correspondence, I noticed that you cite your references. What citation manager do you use? And how do you cite passages - indented and with a vertical line indicating taken from elsewhere - from paragraphs taken from other parts of the internet outside of the current Longecity thread? I find the quoting mechanism self-explanatory for Longecity proper, not not so if I am looking to insert a passage from other parts of the internet.
Feel free to PM me directing me to the best help file, etc, if that helps. I aim to improve the quality of my posts.
From your years experience in the industry, what criteria do you use to vet "reputable brand?' Do you have a short list of acceptable sources?
Criteria would include having been around for a while; showing scientific literacy and modesty in their marketing materials; have passed some third-party testing (CL, Labdoor, Consumer Reports, occasional media exposés, etc); having their GMPs certified by UL, USP, or NSF; being willing to share third-party certificates of analysis; having easily-found US/Canada/EU address and contact information, and being responsive to inquiries; not having FDA Warning Letters (like this) against them; having non-deceptive Supplement Facts and related info (like not playing fast-and-loose with serving sizes or elemental values); and even having professional-looking labels and packaging (if they can't even invest in a decent label, how can they run a clean production facility?).
I'm not saying they should tick all of these boxes, but those are all things I look at and consider valuable.
Thank you for clarifying on raw material vs brand. Sound advice on selection.
At a micro-level, I check with ConsumerLabs, but they don't always have an up-to-date listing for any given supplement. A variety are available from Amazon.com, but presumably this a poor screen!
From your years experience in the industry, what criteria do you use to vet "reputable brand?' Do you have a short list of acceptable sources?
Lysine timing: yes, it's to keep levels up. Not sure what you're asking about "hedging my bets" on lysine: I don't want it competing with other aminos (currently only Trp) for passage of the BBB.
Brands: First, AjiPure is a branded raw material: Thorne and Pure Encapsulations are brands of finished consumer products. I just don't know enough about teh QC of particular retail brands or what they should even be looking for (or whether they'd be looking for it). IT took quite some time for researchers to even identify all the the possible contaminants in Showa Denko's tryptophan that might have been responsible for the EMS crisis, and we still don't know which is the actual culprits decades after the fact. How would one even know where to start on lysine or taurine?
Any reputable brand of GLS should be fine, AFAIK.
Also, I see that you understandably prefer Glucosamine sulphate over glucosamine hydrochloride. What brands do you recommend to source it?
Are you considering resuming glycine , perhaps earlier in the day given your possible somogyi effect, following this recent development @ the ITP: https://onlinelibrar...1111/acel.12953?
The dose used in the ITP study was quite large (8% of diet by weight), was initiated in young adulthood (9 mo), and the effect on lifespan quite modest and uneven (the 6.2% median and 4.5% max figure is averaged over 3 sites, with a much larger effect at UTexas dominating negligible effects in the other two labs); that's not attractive enough for me to consider such a dramatic supplementation program.
As for NR, are you considering suspending or adjusting the dose due to potential loss of methyl groups particularly at conventional doses - a hypothetical concern expressed here https://chrismasterj...amide-riboside/ ?
Some of your stack may partially offset this - e.g., creatine, choline - though not necessarily adequately. That was the short, anecdotal version of a more elaborate version presented in this podcast with Peter Attia: https://peterattiamd...hrismasterjohn/ at around 1:47:15
I'm actually currently taking only 125 mg of NR or NMN 4 d/week, with 250 mg NR 2 d/wk and a one-day weekly holiday, and as you say I have partially offset this potential concern (plus an extremely high dietary intake of folate). I do think it's important to have a decent level of methylating nutrients. I've noted the potential problems of methylnicotinamide, and it's not clear whether/how much that's due to MeNAM being itself toxic vs. it depleting methylating units.
Hi Michael, not sure if you are still checking this thread but why not fisetin?
if you have started , what is your protocol ?
I'm not, yet, though I'm certainly considering it and have almost pulled the trigger more than once. Animals on CR per se accumulate fewer senescent cells as they age (PMIDs 26983960, 20844316, 29575469) — including, apparently, CR humans (PMID 29575469 ) — so my risk:benefit is more favorable than for most. Additionally, the results of a senescent cell ablation study by Dmitry Bulavin at Undoing Aging (I hope video will be up soon) scared the snot out of me; I am awaiting to read the paper and understand more before adopting any senolytic protocol (though fisetin, specifically, seems to be less hepatotoxic than other senolytics, and liver damage was the site of the horror in the Bulavin study).
As to protocol: most people are defaulting to the Mayo Clinic's study protocol of 20 mg/kg/day, orally for 2 consecutive days (often with some effort to enhance bioavailability). The dose seems about right or a little bit high based on either the HED method or true allometric scaling, but on reflection the time period does not: in the rodents, the acute clearance protocol was 5 days, and if anything the idea of "biological time" might suggest a longer period for a longer-lived mammal.
Hi Michael, not sure if you are still checking this thread but why not fisetin?

Are you considering resuming glycine , perhaps earlier in the day given your possible somogyi effect, following this recent development @ the ITP: https://onlinelibrar...1111/acel.12953?
As for NR, are you considering suspending or adjusting the dose due to potential loss of methyl groups particularly at conventional doses - a hypothetical concern expressed here https://chrismasterj...amide-riboside/ ?
Some of your stack may partially offset this - e.g., creatine, choline - though not necessarily adequately. That was the short, anecdotal version of a more elaborate version presented in this podcast with Peter Attia: https://peterattiamd...hrismasterjohn/ at around 1:47:15

HDW, have you tried also to compare other potential biomarkers of aging too, next to the Teloyears, e.g. aging.ai, DNAm, Phenotypic Age etc .. see also the thread on Biological Age. It would be interesting too.
If omnivores get enough preformed vitamin A, than the US must be a nation of vegetarians (just joking).
51% of adults there are estimated from their food-intake to remain below their average daily requirement of vitamin A! The nation with the comparatively highest industrial meat production in this world.
But anyway. Michael, do you know how many month after continous supplementation 'serum retinol and RBP don't seen to be reliable indicator of vitamin status'? Couldn't find it. Because for deficiency it seems:
When dietary vitamin A is provided to vitamin A-deficient children, plasma retinol concentration increases rapidly, even before liver stores are restored (Devadas et al., 1978; Jayarajan et al., 1980). Thus, a low concentration of plasma retinol may indicate inadequacy of vitamin A status, although median or mean concentrations for plasma retinol may not be well correlated with valid indicators of vitamin A status.
In my case I supplemented for years, and intake did reflect in serum levels:
(retinol 425-831; RBP 30-60 lab normal ranges)
year vitA RBP A/RBC intake(avg. for previous 3 years)
µg/l mg/l ≥7 µg/d
2012 501 44 11.4 1,3
2015 597 53 11.4 5,4
2018 705 47 14.9 6,7
Calculated (though already many years ago) that I got in average about 0.13 µg/d retinol from diet, and in avg. about 4.6 µg/d from supplements. Beta-carotene 1.5 µg/d RE from supplements, and 1.3 µg/d RE from diet.
Now with serum 25(OH)D probably few would doubt the validity of this test, because in 2012 it took me double the intake for reaching half the serum levels, than 5 years later in 2018. Simply too many co-factors posibly affecting absorption and metabolism. While preformed vitamin A is still widely seen in something as a mysterious limbo.
Even without health issues, the study finding up to 50% of the population having difficulty in converting beta-carotene into vitamin A, would at least have me enough concerned, to have serum retinol tested.
"Issues" doesn't mean meaningful issues, and omnivores of course get preformed vitamin A already. In any case, as I've pointed out before, serum retinol and RBP don't seem to be reliable indicators of vitamin A status.
I really would like to see the peer reviewed study suggesting there is one for rich humans on this planet.

With all due respect, but Vitamin A for European inhabitants is totally overkill. There's an overdose of dairy-intake and dairy-use in our daily consumption patterns here as it stands. Besides, if not from dairy, we have carrots, pastinaak, not to mention the eggs, liver, fish people eat a lot of here. We don't need Vit A supplemented at all.
Or, better put:
If you can pay for regular use of supplements, you probably consume enough foods with vitamin A already. Or you're living a very strange hermit lifestyle or something like that, but a deficiency, I really would like to see the peer reviewed study suggesting there is one for rich humans on this planet.

I'd add some Black Pepper with the Turmeric, as Piperine greatly enhances the absorption of curcumin into the bloodstream.
In fact, peppers, in genral, are known as overall "enhancers" to any primary drug/supplement they may be coadministered with. Without piperine from the BP, turmeric is very poorly absorbed and, as a result, you could be missing out on many of its advantages.
Great stack. *thumbs up*
Full'a sugar, and several of the mechanisms for CVD protection from wine involve the alcohol.
IAC, I actually quit wine last October, after reconsideration of the epidemiology, particularly the nature of the observed stable low-level drinkers. Not going to detail that now .
Here's some more bad news about glucosamine: it has bad effects in both the normal and injured intervertebral discs of animal models, and at least in vitro, there are other problems associated with glucosamine.
Effects of Oral Glucosamine on Intervertebral Disc Matrix in an Animal Model
https://www.thespine...0776-0/abstract
Glucosamine supplementation demonstrates a negative effect on intervertebral disc matrix in an animal model of disc degeneration.
https://www.ncbi.nlm...pubmed/23324939
Glucosamine promotes longevity by mimicking a low-carb diet
https://www.longecit...-low-carb-diet/
Michael, do you have any concerns about the long-term safety of glucosamine? Some say that there's a theoretical potential for kidney and eye damage.
Oral glucosamine increases expression of transforming growth factor β1 (TGFβ1) and connective tissue growth factor (CTGF) mRNA in rat cartilage and kidney: implications for human efficacy and toxicity.
https://www.ncbi.nlm...pubmed/21466783
Hm. Your citation seems far too preliminary to raise concern (they don't even have protein levels in the kidney, and nothing in the eye); however, you triggered me to dig, and I see these two studies finding a rise in IOP with glucosamine. The second study, which is more robust in design, only finds a rise because of a mixture of a lower baseline (reversion to the mean?) and some post hoc fiddling, and "Although mean rise of IOP was statistically significant in the glucosamine group, more than 2 mm Hg rise in IOP was also more in the treatment group (34% of those receiving treatment vs 12.5% of patients on placebo)." And it was done in Iran.
However, even a suggestion of a risk may not be worth it to some people, especially if their inflammation is already low or they have reason to think they're at risk of glaucoma.
It'd sure be nice to have this done more robustly, and also to see some epidemiology on glucosamine supplement users.
Michael, do you have any concerns about the long-term safety of glucosamine? Some say that there's a theoretical potential for kidney and eye damage.
Oral glucosamine increases expression of transforming growth factor β1 (TGFβ1) and connective tissue growth factor (CTGF) mRNA in rat cartilage and kidney: implications for human efficacy and toxicity.
https://www.ncbi.nlm...pubmed/21466783
Thank you for your suggestions, both of you! I will drop a few based on your recommendations and look into the rosmarinic acid. Never heard of that one! I feel great on this stack, but then I've never had any health issues or complaints. I'm thinking long game here. I very much appreciate the input!
might think about calcium carbonate/magnesium/potassium bicarb three times a day or at least at the end of a workout or during and in the late afternoon
In general, these might be good for preventive but when you are really suffering or have autoimmune problems you will have to change these around.Like increase them all or selectively.

Maybe consider leaving out the ALC, it probably contributes to inflammation by nourishing gut microbes that are best kept in check. Add egcg, reshi and, carnosine. The nicotinamide riboside and pterostelbene are super awesome. I would drop the resveretrol if you are taking pterostelbene. I have reservation about taking PQQ and nicotinamide riboside together. The B complex should be liquid and sublingual. Oh yes.. also a rosmarinic acid polyphenol supplement may be something to look into. It is likely gonna be very good for your skin by preventing AGE crosslinks.

It looks like one of the key drivers of inflammation rising in the aging human might be the release of mitochondrial DNA into the bloodstream, which is then recognized as bacterial DNA and attacked by leucocytes. See the following papers:
'The path from mitochondrial ROS to aging runs through the mitochondrial permeability transition pore'; and
'BAK/BAX macropores facilitate mitochondrial herniation and mtDNA efflux during apoptosis'.
Apologies, I am new to Longecity and am not allowed to post hyperlinks.
Personally I think it is a lack of replicative ability in aging proliferative cells that is the source of the problem, and that a blockade on the inflammatory cascade can only delay the inevitable rather than fully rejuvenate - but this might be the best we have until we manage to restore cells' proliferative ability.

Michael, I have yet a few more questions: on k2, is there really a need to supplement it when one gets sufficient amounts of it (or k1) on a diet? Whether it´s mk7 or mk4? If so, what is the minimal required dosage? Especially for someone my age?
And regarding CR; is it also really making one live longer? So far I have read different evidence upon it on this site. Some say it has been shown to increase lifespan in animals, but not in humans. Perhaps it will only increase the quality of one´s phenotype?
But constantly CR´ing can´t be healthy right? If one does so he/she will continue to lose weight until he/she practically dies of starvation. My BMI is already most of the time in between 17.5-19.5, as of now it is about 17.5. I think I´m already CR´ing without me knowing it as I have lost some weight. You can´t encourage people to keep continue CR´ing until they become hospitalized?
And have you ever looked into coleus forskohlin for increasing BMD? It seems to be completely safe. DNA damage, cytotoxicity, general toxicity, liver damage and case studies all gave negative results. The only caveats I could fine is a study which noticed genotoxicity in Allium cepa (onions). It also raised heart rate 16% in a human study. But I´m not sure it´s a negative thing per se, as coffee also seems to raise heart rate, which you also take (though I´m not sure if decaf coffee raises heart rate). It might be a little bit undesirable when looking at it from a longevity perspective. But I´m not qualified enough to make this definitive conclusion. One study even noticed it being promising for cancer: http://onlinelibrary...320622/abstract
Greger is not a reliable source of health information.
We will see in a short moment. Even though we started with CoQ10, let me first address vit D.
His argument here is based on a mixture of (a) older meta-analyses of studies on single outcomes and not individual patient-level data, and (b) the paleo-adaptationist fallacy that "natural" levels are better.
No, Greger actually said the opposite at 3:05; that the natural level actually is not the optimal level per se. So no ´paleo-adaptionist´ fallacy here.
"something, dont quite remember was a long time ago" is not a good citation. IAC, this is a painstaking individual patient-data meta-analysis of eight independent prospective cohort studies from Norway, Germany, Iceland, Denmark, and the Netherlands, not some single study of "Scandinavians."
I looked it up again, and let me summarize by giving a short chronogical history on vit D:
https://nutritionfac...recommendation/
First this video (from 2011) at about 1:01 shows about >80-90nmol/L is where your body will not be putting more vit D in circulation, about right in the middle where your conclusion of 75-100nmol/L is.
https://nutritionfac...vitamin-d-bate/. Then his conclusion here is 2000IU seems to be best for people in general. Off course, like you pointed out in your ´patient-level data´, the 2000IU is just an average. Some need more or less. You yourself take in about 500-1000IU, but you could be getting more sunlight than the people in Greger´s cited study did. Or you might be taking it in with your meals, which contributes to higher absorption.
However, this is a very old video of doctor Greger from December 2011. The same link also states an ideal of 80nmol/L at 1:27, which is what your study also cites.
Now is a more recent video from 2016. One of the statistics in this video looks remarkably similiar to the one you cited: https://nutritionfacts.org/video/how-much-vitamin-d-should-you-take/. However, this one is outdated. New data in this video shows about >135nmol/L is better than 80nmol/L. Why? Because some of these vit D studies are based on Scandinavian cod liver supplements, which contributed to increased mortality risk due to their vitamin A content, which was beyond the upper dosage. So the U-shaped curve is outdated.
Note the meta-analysis study you stated on vit D cites: ´European consortium of eight prospective studies, including seven general population cohorts´ So this study probably was from these cod liver studies were mostly from Scandinavian countries.
From here on I will just advise you to watch the entire video. After you´re done, we arrive at the video I linked earlier. Please watch this one again, and what I said earlier will make more sense now:
https://nutritionfacts.org/video/the-optimal-dose-of-vitamin-d-based-on-natural-levels/
I said 3:12 before, but I meant to say the study at 3:18. 5000IU pills make more sense now. Perhaps even 10000IU might be better on days without any sun. But it depends on several variables. For some 5000IU might be more than enough, or even 10000IU, just like Greger cited in some of his videos on vit D.
Now on CoQ10.
Does he provide direct evidence of this happening in vivo in aging mammals, or is this the usual mechanistic speculation based on in vitro nonsense? And if so, does he provide direct evidence that this happens in CR animals (as noted, that's why I'm taking it), or alternatively that it is sufficient to counteract the "normal" age-related decline?
Did you watch the video (entirely)? At 2:30 he shows a study which shows mammals can produce ATP themselves after consuming chlorophyll compounds. Or you can read the study yourself: https://www.ncbi.nlm.nih.gov/pubmed/24198392
And at 3:47 he shows a study which states our bodies can produce CoQ10 after sunlight exposure. Or view this study here yourself: https://www.ncbi.nlm.nih.gov/pubmed/22928808
Whether you´re doing CR or not, as long as you eat chlorophyll containing foods and expose your body to the sun, your body will produce CoQ10. I agree sun exposure is carcinogenic, that´s why I take vit D mself, but I guess some sun exposure is unavoidable right? Why not make good use of it? I couldnt figure out though how much was produced, but perhaps you could figure it out?
They're only moderately difficult to obtain. Get a prescription or order from reliable online pharmacies.
Also in the Netherlands? I looked online for any website but couldn´t find any.
Then on the carninutrients: I actually agreed with you. To be honest, I was pushing you a bit in order to get a response. I myself supplement with carninutrients as well for a few months now: beta-alanine, taurine, carnitine and creatine.
However, I did some research some time ago and found out carnitine, taurine and carnosine aren´t a problem in those who take in high amounts of protein every day (~.7g-.8g< protein per pound). Then our bodies would synthesize all we need. There are also some sources claiming our bodies can only synthesize up to 1g of creatine per day, when we need 2g total each day. But I am a bit sceptical of this, considering sites make very distinct claims about creatine and there being no site which accurately lists all creatine sources. It´s also pretty weird no amino acid except creatine would be a problem. I think it´s obvious why I think this is weird.
You do seems to be aware of the relationship between choline and TMAO. I haven´t looked into the choline studies you told about, will look into it. However, there is some evidence vegetarians aren´t getting enought carnitine either (when they take in only moderate amounts of protein, like 70-80 grams a day):
https://www.ncbi.nlm.nih.gov/pubmed/2756917; https://www.ncbi.nlm.nih.gov/pubmed/21753065;
Would you consider supplementing it now as well just like choline, even though there is a TMAO connection?:
https://nutritionfac...mao-connection/. I mean, carnitine should be as essential, just as choline after all.
I also have a little bit extra info about it in the following video, please read my comments: https://nutritionfac...in-supplements/
Loaded with omega-6: no, thanks.
Is there a specific reason you avoid omega 6? Omega 6 is only a problem if you eat it with omega 3, in which case the omega 3 gets ´behind in the line´ of what your body will use fas DHA/EPA. Just consume your omega 3´s first every day, then only omega 6 later. Or simply supplement with a sufficient DHA/EPA omega algae pill.
The bioavailability of Zn in wheat bran is extremely low. 2 T of wheat germ contains 1.8 mg Zn, 0.8 mg omega-6, and 121 mg of phosphorus, plus
Wheat Germ Agglutinin: no, thanks.
I said bran/germ as I was quick in my response, but the following links shows 100g wheat germ contains about 14-12mg, which is pretty significant: https://www.healthal...icles/zinc.php; http://nutritiondata...0000000-w.html. Toasted wheat germ even has 17mg.
And I don´t seed what´s wrong with lectins like WGA. They even have many benefits for our bodies: http://www.sciencedirect.com/science/article/pii/S0733521014000228. As far as I know, when lectins show negative effects, they either use high dosages or use unhealthy populations. Soy isovlavones don´t scare me for this reason, as gynaecomastia only was perceived in case studies involving at least a kilo of soy products daily.
The only one who seems to worry about agglutinin is Mercola, who is nothing more than a witch doctor in my eyes. He only wants to sell his products, unlike Greger who established a non-profit site where procedures goes towards charities.
Although a long-term prospective epidemiological study did find an association between Ginkgo use and slow cognitive decline, its power is limted by only requiring one reported intake at any of ten follwups assessments over the course of 20 yearas (1), whereas two well-done clinical trials (2,3) found no benefit. That's not a good reason for putting a concentrated phytochemical into your body for decades.
Well, never mind the ginkgo now. I just found out ginkgo should be avoided, read about what I typed here:
http://www.longecity.org/forum/topic/98805-known-negative-side-effects-on-certain-supplementsherbsspices/page-2#entry837103
But if a certain supplement is safe, I see no reason why long-term supplementation should be harmful. Whether it is a certain tea, herb, spice or regular food.
Antioxidants, shmantioxidants: that canard should have died in 1992. I'm not aware of any actual health benefits of any of these listed substances in normal, otherwise-healthy aging mammals after oral administration. Can you cite any (with primary scientific citations)?
Don´t have one at hand. But it´s handy for anti-aging and stress as far as I know. Here´s a handy startpage on it:
https://nutritionfacts.org/topics/antioxidants/
Never mind c60, PQQ and NMN, I decided I have no interest in them anymore. However, I do have a couple of questions for you I wandered about:
1) any reason why you´re vegetarian and not omnivorous or whole-food plant-based/vegan? When I looked at your diet I couldn´t spot any animal products though.
2) Are you aware of more people who list their diet and supplement regimen on this or another site in detail like yourself?
3) I need some help with niacin. RWhigham commented in this post something about niacin/niacinamide perhaps decreasing lifespan:
http://www.longecity.org/forum/topic/79920-nicotinamide-without-the-riboside-nicotinamide-by-itself-any-good/. Is this a typo?
And you yourself once said it Increases chance for diabetes. However, another post mentioned blood sugar is only raised temporarily. After same use this blood sugar rise will eventually disappear.
Is 500mg a sufficient dose or is 1g a lot better? I cant find any good info on it. Do take I´m only 24 years old, so I need less than someone older.
4) Ever thought about taking heart rate lowering supplements like valerian or adaptogens at moments of stress? Sure beats lavender, which has been associated with gynaecomastia (see my link about negative side effects linked earlier).
5) Any reason why you dont take spices like dill, chervil or cardamom?
6) Do you know anything about supplementing bromelain? Anything good or bad?
Final, are you one of the ´makers´ of this site? I gotta say I like the site and I thank you for it! :D
EDIT: here is your link about choline: https://www.crsociet...or-vegetarians/. And this is the one of veganhealth.org I was talking about: http://www.veganhealth.org/articles/choline. The article of veganhealth.org contains 5 of the 7 sources your link cites. It has 27 total sources however, also on a few other subjects. The two sources it doesn´t contain are xciv and xcv. I haven´t looked properly at it yet, but you might want to check it out yourself. It´s interesting to see however how they both arrive at different conclusions. Veganhealth.org doesn´t hold any bias, Jack Norris is more than happy to supplement when there is enought evidence to the contrary. He already supplements some nutrients.
I also just noticed you sometimes take 750mcg of melatonin. You can also eat an ounce of goji berries for about 15mcg of melatonin: https://nutritionfac...s-for-insomnia/. Because melatonin is potent it can increase blood levels 50-fold in the body, so one can get about 750mcg of melatonin per 1 ounce of goji berries.
I noticed Darryl has some info on phosphatidylcholine you might be interested in to read: https://nutritionfac...omething-fishy/
Michael, there is a video on nutritionfacts.org which tells how our bodies can produce CoQ10 on our own (hint, you would have to eat green leafy vegetables and get some sun afterwards): https://nutritionfac...oq10-naturally/
Greger is not a reliable source of health information. Does he provide direct evidence of this happening in vivo in aging mammals, or is this the usual mechanistic speculation based on in vitro nonsense? And if so, does he provide direct evidence that this happens in CR animals (as noted, that's why I'm taking it), or alternatively that it is sufficient to counteract the "normal" age-related decline?
IAC, sun exposure is a carcinogen. I'll take the pill. Ditto on vitamin D.
Too bad metformin, rapamycin and acarbose seem impossible to obtain.
They're only moderately difficult to obtain. Get a prescription or order from reliable online pharmacies.
And why no n-acetyl glucosamine but sulphate/sulfate?
The cited studies used GLS, not NAG.
On the Vit D, I looked into it a long time ago but the conclusion was that the study you reference was not legit (based on people taking in fish in Scandinavia or something, dont quite remember was a long time ago).
"something, dont quite remember was a long time ago" is not a good citation. IAC, this is a painstaking individual patient-data meta-analysis of eight independent prospective cohort studies from Norway, Germany, Iceland, Denmark, and the Netherlands, not some single study of "Scandinavians."
The video had a different conclusion on that (3:12): https://nutritionfac...atural-levels/This is why I personally take 10000IU on days without sun and 5000 IU on days with some sun in winter of few in summer.
Greger is not a reliable source of health information. His argument here is based on a mixture of (a) older meta-analyses of studies on single outcomes and not individual patient-level data, and (b) the paleo-adaptationist fallacy that "natural" levels are better.
Carninutrients: why do you take taurine and beta-alanine in such high doses? Taurine barely offers any benefits for as far as I´ve read and omnivores have an average intake of 100-400mg as I have read and about 50-300mg for beta alanine + 36,5% of b-alanine is carnosine so up to 822mg should be sufficient (sorry, no direct sources to back this up as I haven´t safed them but you can probably find the sources yourself).
Taurine: see my paragraph on this, beginning "AjiPure Taurine: Absent in vegetarian diet;" and references (32) and (33) on benefits and dose. Beta-alanine: because those are the doses used in clinical trials.
No references, no argument.
Carnitine has been shown to not raise TMAO levels in vegans though: https://nutritionfac...ao-connection/
That's what's reported, yes — but (a) it's based on a single "carnitine challenge consisting of co-administration of 250 mg d3-(methyl)-carnitine and an 8-ounce sirloin steak" in a small sample size (n=23), and (b) presuming it's real, the reason why is presumably because carnitine is so low in the veg(etar)ian diet that bacteria that avidly metabolize it don't get the fuel they need to grow to substantial numbers in the gut. If you obviate that situation by taking a supplement every day, you'll be feeding those bugs and their numbers will expand accordingly, leading to omnivore-level TMAO production.
Plus, carnitine probably raises sperm quality (see the comments I made in the link; user: Leon)
Bonus! By not taking it, I get a little background birth control .
Veganhealth.org has a page on choline and says the 450/550mg per day is based on a single old study.
If it says that (link, don't claim), it's wrong: the DRI is supported by multiple studies, including those I cited in my linked "supplements for vegetarians" post.
As user Darryl also pointed out, 170-300mg might be sufficient supplemented with betaine (easily obtained from wheat bran).
Betaine raises TMAO. Wheat bran is not remotely a high enough source of betaine, and betaine not an adequate substitute for choline, to make up the gap.
Zinc: wheat bran/germ offer insane high amounts of zinc.
The bioavailability of Zn in wheat bran is extremely low. 2 T of wheat germ contains 1.8 mg Zn, 0.8 mg omega-6, and 121 mg of phosphorus, plus
Wheat Germ Agglutinin: no, thanks.
Pumpkin seeds and sesame seeds as well, but lower. Tryptophan can also be easily obtained from diet: http://nutritiondata...0000000000.html
Loaded with omega-6: no, thanks.
Is there a specific reason you haven´t looked into spices and herbs? Ginkgo biloba might hold some promising effects for cognition and turmeric, sumac and cloves f.e. are very high in antioxidants. Amla (powder or berry/dried berry) and astaxanthin are also extremely high in antioxidants.
Although a long-term prospective epidemiological study did find an association between Ginkgo use and slow cognitive decline, its power is limted by only requiring one reported intake at any of ten follwups assessments over the course of 20 yearas (1), whereas two well-done clinical trials (2,3) found no benefit. That's not a good reason for putting a concentrated phytochemical into your body for decades.
Antioxidants, shmantioxidants: that canard should have died in 1992. I'm not aware of any actual health benefits of any of these listed substances in normal, otherwise-healthy aging mammals after oral administration. Can you cite any (with primary scientific citations)?
Any reason for not supplementing PQQ, NMN or c60?
PQQ: I'm aware of no evidence of benefits in normal, otherwise-healthy aging mammals in vivo after oral administration. Can you cite any (with primary scientific citations)?
NMN: I'm taking NR; I don't think we know enough to think that either is better at this point, or that taking both is better than taking one at the same total molar dose. NR's supply chain is clearer, it has a monographed analytical method, and it's cheaper.
c60: a lot of hype over a badly-done, retracted animal study that doesn't pass the laugh test. There is at present no evidence of benefits in normal, otherwise-healthy aging mammals in vivo after oral administration — or can you cite any (with primary scientific citations)?
References
1: Amieva H, Meillon C, Helmer C, Barberger-Gateau P, Dartigues JF. Ginkgo biloba extract and long-term cognitive decline: a 20-year follow-up population-based study. PLoS One. 2013;8(1):e52755. doi: 10.1371/journal.pone.0052755. Epub 2013 Jan 11. PubMed PMID: 23326356; PubMed Central PMCID: PMC3543404.
2: van Dongen M, van Rossum E, Kessels A, Sielhorst H, Knipschild P. Ginkgo for elderly people with dementia and age-associated memory impairment: a randomized clinical trial. J Clin Epidemiol. 2003 Apr;56(4):367-76. PubMed PMID: 12767414.
3: Snitz BE, O'Meara ES, Carlson MC, Arnold AM, Ives DG, Rapp SR, Saxton J, Lopez OL, Dunn LO, Sink KM, DeKosky ST; Ginkgo Evaluation of Memory (GEM) Study Investigators. Ginkgo biloba for preventing cognitive decline in older adults: a randomized trial. JAMA. 2009 Dec 23;302(24):2663-70. doi: 10.1001/jama.2009.1913. PubMed PMID: 20040554; PubMed Central PMCID: PMC2832285.
Michael, there is a video on nutritionfacts.org which tells how our bodies can produce CoQ10 on our own (hint, you would have to eat green leafy vegetables and get some sun afterwards): https://nutritionfac...oq10-naturally/
On the Vit D, I looked into it a long time ago but the conclusion was that the study you reference was not legit (based on people taking in fish in Scandinavia or something, dont quite remember was a long time ago). The video had a different conclusion on that (3:12): https://nutritionfac...atural-levels/ This is why I personally take 10000IU on days without sun and 5000 IU on days with some sun in winter of few in summer.
This link states humans get in an average of a bit lower than 1mg of lithium a day up to about 3mg: https://getfit.jilli...thium-1831.html Vegetables and grains seem to be high in it.
Carninutrients: why do you take taurine and beta-alanine in such high doses? Taurine barely offers any benefits for as far as I´ve read and omnivores have an average intake of 100-400mg as I have read and about 50-300mg for beta alanine + 36,5% of b-alanine is carnosine so up to 822mg should be sufficient (sorry, no direct sources to back this up as I haven´t safed them but you can probably find the sources yourself).
Carnitine has been shown to not raise TMAO levels in vegans though: https://nutritionfac...ao-connection/
Plus, carnitine probably raises sperm quality (see the comments I made in the link; user: Leon)
B12 might be better in cyanocobalamin form as Michael Greger often suggests as there is more research to support it and the other forms don´t work for every person. It´s also the cheapest and safest form. Greger suggests 2500mg a week but if you look at this video, 3750 should be closer to the ideal dosage: https://nutritionfac...of-vitamin-b12/
Veganhealth.org has a page on choline and says the 450/550mg per day is based on a single old study. As user Darryl also pointed out, 170-300mg might be sufficient supplemented with betaine (easily obtained from wheat bran).
Zinc: wheat bran/germ offer insane high amounts of zinc. Pumpkin seeds and sesame seeds as well, but lower. Tryptophan can also be easily obtained from diet: http://nutritiondata...0000000000.html
Is there a specific reason you haven´t looked into spices and herbs? Ginkgo biloba might hold some promising effects for cognition and turmeric, sumac and cloves f.e. are very high in antioxidants. Amla (powder or berry/dried berry) and astaxanthin are also extremely high in antioxidants.
Too bad metformin, rapamycin and acarbose seem impossible to obtain. Any reason for not supplementing PQQ, NMN or c60? And why no n-acetyl glucosamine but sulphate/sulfate?
I hadn't run across the Vitamin A info. Might you suggest a link?
If there's a way to take more Vitamin D3 and keep the dosing risk low, I'm in to do it.
For example the point of view by Chris Masterjohn.
If you remember slimjohn, he also has given it lot of thought on his forum, for example here. (needs signing up, but is for free)
Personally on Pauling's therapy for many years, reached his recommendation of 25.000 IU preformed vitamin A only recently. Since which my infrequent psoriasis outbreaks have completely ceased.
Then there is Dr. Coimbra from Brasilia, which uses REALLY large doses of vitamin D against MS, and describes all precautions he recommends. A selection of texts for example here.
Enjoy.
Various NF-kB Herbal Inhibitors -- Daily Fisetin, Feverfew, Berberine, Bitter Melon, Propoulis
Fisetin, Feverfew, Berberine, Bitter Melon, are all strong P450 3A inhibitors. Propoulis inhibits P450 1A2 only. 3A is the most important
While stacking NF-kB inhibitors it might be wise to avoid stacking a lot of P450 inhibitors. P450 is one of the ways the liver detoxes the things we eat.
Everyone who can should check their P450 genetics. Defects are common.
No effect on P450 3A
AshwagandhaAstragalusCurcuminEleuthero senticosus - Siberian EleutheroIcariin/Horny Goat WeedMetforminNettle RootPQQ
P450 enhancers
Aspirin
AstragalusEleuthero senticosusNettle Root (some other not 3A)P450 inhibitors - some of these (at the top) are very strong, some are not. This list shows how easy an herbal stack could inhibit P450Grapefruit juiceBerberineNaringenSchizandraQuercetinBergamotBitter MelonAndrographisResveratrolPterostilbeneFisetinEGCG extract - a fairly weak 0-20% effect at 800 mg/dMagnolia/HonokiolGinkgoBacopaWild YamBilberry - and most berriesMilk ThistleGrape seed extractGingerAloe VeraPomegranatePropoulis- inhibits 1A2 only
Thank you very much RWhigham for the info... I will look into this and be back with comments when I have them.
20.000 IU D3 ongoing is quite a dose. What 25(OH)D3 levels to you get with that? Or aim at?
Do you take any retinol? Since vitamin A and D3 and K2 all seem to support each other, and prevent toxicity of each taken at high doses. Did you ever test your serum retinol and retinol binding protein?
Thanks.
Hi pamojja... I remember you from years ago at Dr Davis' Track Your Plaque forum. I posted there as wccaguy.
I understand it's a large dose. I supplement with Vitamin K.
I get my Vitamin D3 blood tested regularly. I've only tested Vitamin D3 over a hundred once.
I hadn't run across the Vitamin A info. Might you suggest a link?
If there's a way to take more Vitamin D3 and keep the dosing risk low, I'm in to do it.
Thank you for the information.
Because (a) rapamycin is really a pretty risky drug to take experimentally (at least at levels likely to be effective, assuming the rodent data does indeed translate — see discussion here and this followup) and (b) there seems to be surprisingly little advantage to starting rapa earlier in life vs. later, perhaps because its beneficial effects become more relevant in opposition to secondary aging processes or because the mixture of deleterious to beneficial effects shifts with the changing aging milieu — or perhaps simply because of changing pharmacokinetics, since in the mice at least plasma levels at a given dose are much higher in aged vs. young animals.
So I feel I've got some time, and we'll certainly know a lot more in a few years.
The stupidest thing in the universe is a life extensionist dead of the long-term toxic effects of his experimental fountain-of-youth pill.

Hi Michael,
I'm curious as to why you don't take Rapamycin considering that at top of your post you state "whereas we now have extremely convincing evidence for rapamycin" as regards to supplements.
I'm thinking of getting my parents, who are in their seventies, on rapamycin (once weekly 5mg) + metformin as a stepping stone to the availability of senolytic treatments.
Thanks,
Chris
I like the entire suite of functional iron markers to be very low-normal. Absent such "full-spectrum" testing, low-normal ferritin.Michael,
"my iron stores are still right where I want them to be."[/size]
What levels e.g. of ferritin do you consider optimal for most people?
Michael,
"my iron stores are still right where I want them to be."
What levels e.g. of ferritin do you consider optimal for most people?

Various NF-kB Herbal Inhibitors -- Daily Fisetin, Feverfew, Berberine, Bitter Melon, Propoulis
Fisetin, Feverfew, Berberine, Bitter Melon, are all strong P450 3A inhibitors. Propoulis inhibits P450 1A2 only. 3A is the most important
While stacking NF-kB inhibitors it might be wise to avoid stacking a lot of P450 inhibitors. P450 is one of the ways the liver detoxes the things we eat.
Everyone who can should check their P450 genetics. Defects are common.
No effect on P450 3A
P450 enhancers
Aspirin

Be careful with your vitamin C and E dosages, too. If you are taking AREDS2 Preservision twice a day you could cut back to once a day, reduce any risks of chronic vitamin C, E and zinc overdose, and likely reap most of the benefits of the lutein/zeaxanthin
Looks like a killer stack! How do you feel on it? Have you tried going a month without it and making a comparison?
My recommendations:
- Resveratrol results have been disappointing, and it can be expensive. You could consider dropping it unless you think it makes you feel noticeably better.
- Alpha Lipoic Acid doesn't have to be a daily supplement, maybe just take it when you are particularly stressed or doing something stressful.
- Acetyl-L Carnitine could be dropped back to 100-500 mg per day.
- Schisandra could be dropped, unless you think it makes you feel noticeably better.
- Ubiquinol could be dropped back to once a week. It seems to be useful as a "top up" but likely not worth a daily supplement unless you're on statins.
- Vinpocetine could be dropped, unless you think it makes you feel noticeably better.
- Turmeric can be switched to a cheap curcumin + piperine supplement. e.g. Doctor's Best
+ Methylene Blue, a low dose (1-10 mg diluted in water, drunk over the day) seems to be a very cheap, safe and medically promising supplement.
+ Sodium Oxybate, if you can get a prescription or join a trial, is a very promising preventative for dementia. Improving sleep depth is vital for mental health.
But serum retinol and RBP don't seem to be reliable indicators of vitamin A status, and I have great night vision, no hyperkeratosis, and my immune system seems highly functional despite all the weirdness around CR immune function studies.
It's just that I trust a cheap retinol and RBP test in my serum more than research in any other. Had these (fat-diet and BMI) also covered, but needed ridiculous high amounts just to normalize my levels.
Nope! I get ≈1/9 of the DRI RDA from retinol, and 5.68 times the DRI RDA for vitamin A as carotenoids from beta-carotene alone, plus lots of alpha-carotene: that more than coveres a genetic variation of up to -69% from the canonical SNP (and we don't know the percentage of slow-converters have been included in the studies used to set the DRI RDA: unless every single one of them had the reference SNP, -69% is a worst-case scenario). Plus, human and animal evidence shows that bioconversion is increased in the face of a high-fat diet (check), and is negatively correlated with BMI (covered).
Thanks. so this study: http://www.fasebj.or...23/4/1041.fulldoesn't concerns you?
I've never seen any compelling case for RBP testing, granted my very large beta-carotene intake and small but nonzero retinol intake. My 25(OH)D3, as I mentioned, is now in the low end of the 30-40 ng/dL range.
20.000 IU D3 ongoing is quite a dose. What 25(OH)D3 levels to you get with that? Or aim at?
Do you take any retinol? Since vitamin A and D3 and K2 all seem to support each other, and prevent toxicity of each taken at high doses. Did you ever test your serum retinol and retinol binding protein?
Thanks.
Michael, as followup on a discussion elsewhere, did you ever test serum retinol and RBP? Also would be interested in you 25(OH)D3, if you would be willing to share.
I'm still searching, but I doubt there is any research of A, D3 and K2 in combination with hard health outcomes yet. Only have my own anecdotal case of being plagued with a number of devastating chronic diseases, and without much to loose, therefore was more than willing to experiment while monitoring. I didn't regret.
However, you might be absolutely right in that the A:D ratio which worked for me, might turn out completely off in a healthy person. Therefore always worthwhile testing serum retinol and retinol binding protein for confirmation. As an example of a very healthy person, what kind of serum levels you get with A and D?
In principle, I'd agree that we'd want to be able to evaluate the whole system working together — but I don't know of any proper data on the subject, even in animals. The studies cited in the posts that you and RWhigham link cite are biochemistry, acute toxicity, and rather speculative inductions (eg, that the reason why trials conducted in the 1930s showed that cod liver oil reduced incidence of common colds and respiratory infections but that a 2004 trial yielded mixed results is that the cod liver oils differed in A and D content, and should have had higher D and lower A than the 2004 trial — or that the reason for low 25(OH)D3 in LEF members is excessive vitamin A supplementation from non-LEF multivitamins, even though the article itself says that "Most Foundation members take the Two-Per-Day or Life Extension Mix multi-nutrient formulas," which by their notions of a correct vitamin A dose do not suffer this problem).
Are either of you aware of any long-term studies in otherwise-normal, aging mammals testing the effects of different ratios of vitamins A, D3, and K2 against hard health outcomes?
Thanks for both comments, only saw them now.
I'm thinking more in line with Chris Masterjohn. And got his ideas confirmed through vitamin A and D serum testing, while aiming at the middle of normal ranges. In that I actually need at least a A to D IU ratio of 2 to 1 (the opposite RWhigham suggests). With the higher intake of preformed vitamin A, always slowly titrating and measuring, also infrequent psoriasis outbreaks have ceased (above 24.000 IU/d). But everyone is different, where only individual testing counts.
The problem I have with all the references you both provide, is that they look completely unrealistically at one vitamin - A or D in isolation only. That's how I never would even think of them, or further excluding vitamin K2 in all their synergistic effects.
You meant Vitamin K2 MK7, right?
To make meaningful comments, we'd have to understand why you were taking these things, and at the dose you're taking them. I see no justification at all for an otherwise-healthy aging person to be taking Olive Leaf Extract, Ashwangandha, or Curcumin. EGCG, Broccoli Sprout Extract, and Garlic Extract are fine, I suppose, but you'd be better taking the actual foods (and green tea pills have been linked to a fair number of cases of liver toxicity, unlike the tea). Your EPA+DHA dose is probably twice as high as it should be. Your vitamin D is also likely way too high: are you having your 25(OH)D tested, and if so, what level are you targeting? See discussion at my stack (and, indeed, see discussion there on supplementation generally).
In response to aribadabar's questions:
I quit IP6 because I have persistently high serum phosphorus (which is bad), and because my dietary IP6/phytate and inositol is already likely at the extreme end of the population (legumes and nuts). Additionally, there was little positive reason to take it, either: I don't have any history of kidney stones, I drink plenty of fluids and have a high-intrinsic-water diet, and no one has yet done a study showing it benefits otherwise-healthy aging rodents or humans. And if it's working by mobilizing NK cells, well, who knows what decades of incessant NK stimulation could do?
I quit the lactoferrin because I finally admitted to myself that there's never really been any good reason to take the stuff. And my iron stores are still right where I want them to be.
Glycine: I decided that I had to stop drinking water just before bed in order to avoid a mid-night trip to the bathroom, which seems like a more sensible way to ensure solid slip than doping myself up with supplements — and I'm reluctant to take it on an empty stomach. Plus, I suspect that it may have been the reason for my occasional bouts of waking up at 3 AM with a pounding heart and a sweat: my hypothesis is that this is due to Somogyi effect, arising from the interaction of glycine-induced insulin secretion with my having CR-associated high insulin sensitivity and low glycogen stores: see here and here. Certainly, I've had none of these episodes in the months since I quit taking it.
The diff' is that PC raises TMAO less than citicoline.
Do we know whether it raises TMAO less per total mg or per mg of choline supplied?
Per mole (properly) of choline supplied. We don't have actual quantification on citicoline, but it's been demonstrated that it raises it, and since citicoline is hydrolyzed in the intestine prior to absorption, the relative amount should be similar to that of choline salts; clean PC barely raises TMA(O) at all, whereas choline salts raise it ninefold.
Decent holistic reasoning, but while Jiaogulan has ben shown to improve insulin sensitivity and reduce HbA1c, it doesn't have any evidence for it's longevity effects. You could pick something like rapamycin, selegiline, metformin, or aspirin for more assured increases in lifespan. I'd even pick reishi, another 'immortality herb' over jiaogulan, but ideally both need to be studied more... I hope we can secure some funding for such research in the near future!
Turmeric + Black Pepper is probably not doing much for you, considering you have a plant-based diet already. The clinically meaninful effects are seen with high doses of mixed curcuminoids, not plain turmeric.
Otherwise... good approach!
OK, let me take these one at a time. First with regard to mushrooms, I agree, which is why I specifically mentioned them in my write up, although I could have gone into more detail. Shiitake and Reishi are fine choices, I recommend a wide variety, and even the plain old cheap white button mushroom is very good for you. Oyster mushrooms contain natural LDL lowering compounds.
With regard to jiaogulan - there are a large number of published studies from reputable sources demonstrating its health benefits, if you take that alone, its pretty logical to assume it would help with longevity, anecdotally, the people groups that consume it daily are known for their comparative longevity (admittedly, that alone is not great evidence). Its very hard to scientifically prove ANYTHING is good for human longevity, we just know what improves biomarkers of health. Mouse studies are interesting but not always relevant.
"You could pick something like rapamycin, selegiline, metformin, or aspirin for more assured increases in lifespan"
I consider these myths, mostly debunked, although still under active scientific scrutiny. There is even less evidence that these will result in longevity than exists for jiaogulan, in fact taking these drugs is more likely to harm an otherwise healthy person. Rapamycin is well known for compromising the immune system and promoting cancer, metformin has an enormous list of negative side effects and has never been shown to increase max lifespans (more on this below). Aspirin is a terrible idea for healthy people (primarily due to increased chance of gastrointestinal bleeding):Aspirin Bleeding Risks Outweigh Benefits - ABC News
"The following critique was authored by a Professor of Applied Statistics at the Open University in the UK ("Professor" is a much more senior position in the UK than the USA, denoting something like a department head), and seems cogent and consistent with a slightly cryptic phrase in the abstract, in which case the study is likely not worth paying much attention to:
Quote
Expert reaction to study looking at type 2 diabetes, metformin and lifespan
The title of this paper itself is not helpful in that anyone reading it might get the wrong idea – this study cannot actually answer the question it poses (“Can people with type 2 diabetes live longer than those without?”) for reasons discussed below, and it sounds almost as if there are grounds to advise people without diabetes to take metformin. But in fact the study isn’t saying that at all.
In the press release, Craig Currie says “People lose on average around eight years from their life expectancy after developing diabetes” and goes on to explain why. So if the life expectancy of people with type 2 diabetes is so much shorter, how on earth can they “live longer than people without the disease”, as the title of the release and the paper both say?
The answer is that the comparison in the paper runs only over the time period when the patients with diabetes were on first-line treatment with metformin, on its own (and there’s a similar comparison involving patients whose first-line treatment is with sulphonylureas). At some point after this first-line treatment starts, many of the patients with diabetes would be switched from metformin alone onto a second-line treatment, and this switch is (or should be) necessary because the diabetes or its effects have got worse. But at that point the comparison in this study simply stops.
So the quote in the press release about an eight year reduction in life expectancy, in people who develop type 2 diabetes, is talking about the entire rest of a person’s life after the diagnosis, including the time when they might be on a more aggressive second-line treatment. But the comparison in the paper is looking only at the time before the treatment changes. ...
[MR: This is evidently what the abstract means by using a "censored followup:" they ONLY looked at deaths occurring WHILE the person was on metformin or sulfonylureas: if your disease progressed, and they added on a secnd drug to bring your glucose back under control, you were simply "censored" out of further followup. This would obviously greatly bias the resulting mortality rates (and note: it is for sure from the abstract that they did not actually look at life expectancy, despite the press release AND the title of the abstract: explicitly , they ONLY looked at mortality rates of people while they were only on one drug (or, during the matched number of years of the nondiabetic controls). This means, by definition, that people who were put on the drug most usually used for the mildest diabetes (metformin) and who remained stable and healthy on it, were being compared to more severe patients at outset (on sulfonylureas), and as soon as they got sick they vanished from the analysis! Comparing even average nondiabetic people to unusually successful diabetics is, from the get-go, comparing elite diabetics to merely average aging people. Returning to the critique:]
The researchers did match the controls with patients with diabetes in certain ways, and in their statistical analysis they try to allow statistically for other differences between the people with diabetes and the controls. But the paper itself points out some issues. The researchers could not take into account certain possible confounders (other variables that might affect the comparison) because they did not have data on them for enough of the controls. Even without that important issue, statistical adjustment for confounders is never perfect. The difference in survival between people with diabetes on metformin, and controls without diabetes, was statistically significant but in fact rather small, and probably within the range where it could be explained by residual confounding ...
Further, the paper itself also points out that people with diabetes are more likely be monitored for, and receive interventions for, problems with the heart and circulation. This extra intervention and monitoring, and the possibility of residual confounding, between them cast huge doubt on the possibility that the better survival in the patients taking metformin, compared to controls without diabetes, was simply because they were taking metformin. ...
http://www.scienceme...n-and-lifespan/
And, as a reminder: metformin has been tested now at high and low doses in normal, healthy mice, and also in a somewhat flawed study in rats, and in no case has metformin increased maximum lifespan;there was a very mild increase in average LS in the mouse studies, which might well be due to residual effects of a diet of lab chow and no exercise." [Credit to Michael Rae on that metformin info].
"Turmeric + Black Pepper is probably not doing much for you"
Like Jiogulan, there is a mountain of scientific evidence for the benefits of small amounts of turmeric in one's diet, among many other things, its a very powerful anti-inflamatory. Slightly off topic, but its also a phenomenal tool for recovery improving postoperative pain and fatigue.
-Gordo
Why did you remove Lactoferrin, Inositol /IP-6 and Glycine from your regimen as per its previous version?
Decent holistic reasoning, but while Jiaogulan has ben shown to improve insulin sensitivity and reduce HbA1c, it doesn't have any evidence for it's longevity effects. You could pick something like rapamycin, selegiline, metformin, or aspirin for more assured increases in lifespan. I'd even pick reishi, another 'immortality herb' over jiaogulan, but ideally both need to be studied more... I hope we can secure some funding for such research in the near future!
Turmeric + Black Pepper is probably not doing much for you, considering you have a plant-based diet already. The clinically meaninful effects are seen with high doses of mixed curcuminoids, not plain turmeric.
Otherwise... good approach!
The diff' is that PC raises TMAO less than citicoline. I don't know which would raise serum choline more, but I prefer PC because it's both safer based on TMAO and I think consuming it this way is more conservative: my far-from-expert understanding is that CDP-choline is quite rare in the diet, being only present as an intermediate in PC synthesis in the CDP-choline pathway.
Do we know whether it raises TMAO less per total mg or per mg of choline supplied?
high intake of preformed vitamin A increases fracture risk.
Ref: Excess Vitamin A Can Thwart Vitamin D
Osteoporosis is caused by a mismatch between vitamin A, D, and K2. The ideal A/D ratio wt/wt is about 5 to 1 which corresponds to an iu/iu ratio of 1 to 2.4 since 1 mg of vitamin A is 3,333 iu and 1 mg of vitamin D3 is 40,000 iu so 5 g to 1 g = (5)(3,333 iu)/40,000 iu = 1 to 2.4 iu/iu
Example: vitamin A retinol at 1,000 iu per day needs 2,400 iu per day of D3.
The "more is better" supplements are ridiculous--a quick look a Amazon show "vitamin A" in 5,000 to 25,000 iu capsules (likely mostly beta-carotene). A 25,000 iu dose of retinol would need to be balanced with 2.4 x 25,000 = 60,000 iu of D3. Perhaps you could take one 25,000 iu vitamin A (as retinol) per month and balance it with 2,000 iu of vitamin D3 daily.
A note of caution on preformed vitamin A. You're right that the acute toxicity of very high levels of retinol has possibly been overestimated, but there is significant evidence that high intake of preformed vitamin A increases fracture risk. The studies aren't totally consistent; notably, studies based on serum levels are far less likely to find an association, but that may be because serum retinyl esters poorly track high dietary intake. Even so, a meta-analysis of prospective studies concluded that both high dietary and high blood retinol are associated with elevated fracture risk.
I will add and subtract to and from the stack over time...
Here's a snapshot of my Teloyears report...

The diff' is that PC raises TMAO less than citicoline. I don't know which would raise serum choline more, but I prefer PC because it's both safer based on TMAO and I think consuming it this way is more conservative: my far-from-expert understanding is that CDP-choline is quite rare in the diet, being only present as an intermediate in PC synthesis in the CDP-choline pathway.
And at the beginning of the 6th year, though with in many respect worse lab results, intermittent claudication symptoms have completely gone for the first time during all these years.
...To summarize - through the synergistic effects of lifestyle modifications, nutrient and herbal extract supplementation it was possible: ...
Interestingly, right after the time intermittent claudication ceased I came across the work of Kelly A. Turner, which summarized pretty well for me in a different context the different realms of lifestyle-modifications possibly involved. Since my stack doesn't talks much beyond point 4 of this list - and supplements alone are definitely not enough against severe chronic conditions - I add her whole list here:
During the course of the study, Kelly identified more than seventy-five factors that cancer survivors said they used as a part of their healing journey. Nine of these factors were used by almost every one of them. They are as follows:
1. Radically change the diet
Let your food be your medicine, and medicine your food (Hippocrates)
- avoid sugar, meat, dairy products and processed foods
- eat lots of fruits and vegetables
- limit to organic food
- drink only filtered water
2. Take control of health
Action is the basic key to success (Pablo Picasso)
- actively participate
- be prepared for change
- resolve resistance
3. Follow your own intuition
In vital matters, the decision should come from the unconscious, somewhere from within (Sigmund Freud)
- listen to body signals
- activate the intuition
- find the right change
4. Take herbs and food supplements
The art of healing comes from nature and not from the physician (Paracelsus)
- help digestion: digestive enzymes, prebiotics and probiotics
- boost the immune system: e.g. Vitamin C, other vitamins (B12, D3, K2), fish oil, trace elements, certain edible fungi, aloe vera; and hormones (melatonin)
- detoxify the body:
- antimycotics (eg olive leaf extract, celery, nettle)
- antiparasitic substances (eg wormwood, yellow root, black nut husks)
- antibacterial and antiviral (eg garlic, oregano oil, Pau d'Arco)
- liver detoxification (eg milk spotted dwarf, dandelion root, sweet tooth root)
- supplements alone is not enough
5. Release oppressed emotions
Anger is an acid which can cause much greater damage to the vessel in which it is stored than to what it pours (Mark Twain)
- disease is blockade
- what are suppressed emotions?
- stress and cancer
- anxiety and cancer
- the waterfall solution
6. Enhance positive emotions
The meaning of life is to be happy (Dalai Lama)
- what are positive emotions?
- what are the positive emotions in the body?
- happiness must be practiced daily
- but one does not have to be permanently happy
7. Allow social support
In poverty and misery, friends are the only refuge (Aristotle)
- experience love
- do not feel alone
- physical contact
8. Deepen the spiritual connection
This is the greatest mistake in the treatment of diseases: that there are doctors for the body and physicians for the soul, where both can not be separated (Plato)
- experience spirituality
- a third kind of love
- the relationship between the physical and the spiritual
- it is important to exercise regularly
- it is important to calm the mind
9. Have strong reasons for life
People say that it is the meaning of life that we all seek. I do not believe that this is what we are really looking for. I believe what we are looking for is an experience of being alive ... (Joseph Campbell)
- placing deep trust in one's inner being
- the mind directs the body
- find one's calling
http://www.radicalremission.com/
This April I finally quit one of my two part-time jobs, because it has become merely a stick it out feat, and below devastating effects didn't change even half an hour in working-ability or sleeping needs all these years:
What causes the difference in safety between taking the 2 x 420mg PC vs 2 x 55mg citicholine? Would the two result in the same serum choline levels?

Please note that if you only pick any one single thing off this list, pick the CeraVe and focus on good habits mentioned in the description.
What brand of ubiquinol do you use Michael? No love for Mitoq?
I use any reputable brand: it's all Kaneka in the end.
No, no love for MitoQ. First, as I indicated, I'm taking it for physiological replacement, not some pharmacological mito antioxidant effect. Second, it would be foolish at this point to be taking it for some pharmacological mito antioxidant effect, since it's very clear at this point that it has none in normal mammals(1,2) — nor, indeed, is there any other evidence of any benefit in normal mammals, except maybe in skin cream.
References
1: Sakellariou GK, Pearson T, Lightfoot AP, Nye GA, Wells N, Giakoumaki II, Griffiths RD, McArdle A, Jackson MJ. Long-term administration of the mitochondria-targeted antioxidant mitoquinone mesylate fails to attenuate age-related oxidative damage or rescue the loss of muscle mass and function associated with aging of skeletal muscle. FASEB J. 2016 Nov;30(11):3771-3785. Epub 2016 Aug 22. PubMed PMID: 27550965; PubMed Central PMCID: PMC5067250.
2: Rodriguez-Cuenca S, Cochemé HM, Logan A, Abakumova I, Prime TA, Rose C, Vidal-Puig A, Smith AC, Rubinsztein DC, Fearnley IM, Jones BA, Pope S, Heales SJ, Lam BY, Neogi SG, McFarlane I, James AM, Smith RA, Murphy MP. Consequences of long-term oral administration of the mitochondria-targeted antioxidant MitoQ to wild-type mice. Free Radic Biol Med. 2010 Jan 1;48(1):161-72. doi: 10.1016/j.freeradbiomed.2009.10.039. Epub 2009 Oct 23. PubMed PMID: 19854266.
It's really not clear that oral arginine substantially increases growth hormone secretion, particularly in physically active people or in combination with exercise:
The Ergogenic Potential of Arginine
It is well documented that the infusion of arginine stimulated growth hormone secretion from the anterior pituitary [5, 7]. This increase in growth hormone secretion from arginine infusion has been attributed to the suppression of endogenous somatostatin secretion [8]. The amounts of arginine infused to elicit the growth hormone response ranged from 12 grams to 30 grams. The clinical investigations of oral consumption of arginine and its impact on growth hormone release are not in agreement. When arginine (1.2 g) was ingested along with the amino acid lysine (1.2 g) in young males, peak plasma growth hormone concentrations increased 8-fold at 90 minutes post-ingestion [9]. However, when arginine and lysine were ingested alone at the same doses, there was no corresponding increase in plasma growth hormone. Suminiski and associates [10] reported that the ingestion of arginine (1.5 g) and lysine (1.5 g) resulted in a 2.7-fold increase in plasma growth hormone concentrations in resistance trained males. Colombani et al. [11] supplemented marathon runners with 15 g arginine aspartate for 14 days before a marathon run. On the day of the marathon, blood samples were taken shortly before the run, after 31 km, at the end of the run, and after a recovery period of two hours. The researchers found that growth hormone concentrations were elevated during a marathon run to a greater degree than exercise would elicit alone.
Other studies using either resistance trained or physically active individuals showed no increases in plasma growth hormone concentrations following arginine supplementation. When resistance trained males consumed approximately 8 grams of arginine daily for 17 days there was no associated changes in growth hormone concentrations [12]. Similarly, Lambert et al. [13] gave male bodybuilders 1.2 g of arginine and 1.2 g of lysine. This supplementation did not induce a statistically significant increase in serum growth hormone concentrations over a 3 hour period. In a recent review, Chromiak and Antonio [4] highlighted several factors that appear to modify the growth hormone response to amino acid administration. These include training status, age, sex, diet, and time since last meal. Also, the growth hormone response to amino acid ingestion may be reduced in exercise-trained individuals [4]. These authors concluded that the practice of consuming specific amino acids, including arginine, during or after exercise does not appear to be effective [4].
Growth hormone, arginine and exercise
Recent studies have shown that resting growth hormone responses increase with oral ingestion of L-arginine and the dose range is 5–9 g of arginine. Within this range there is a dose-dependent increase and higher doses are not well tolerated. Most studies using oral arginine have shown that arginine alone increases the resting growth hormone levels at least 100%, while exercise can increase growth hormone levels by 300–500%. The combination of oral arginine plus exercise attenuates the growth hormone response, however, and only increases growth hormone levels by around 200% compared to resting levels.
Summary: Exercise is a very potent stimulator of growth hormone release and there is considerable research documenting the dramatic growth hormone rise. At rest oral L-arginine ingestion will enhance the growth hormone response and the combination of arginine plus exercise increases growth hormone, but this increase may be less than seen with exercise alone. This diminished response is seen in both in both younger and older individuals.
Additionally, although it's been tested in unhealthy people, trials of chronic arginine supplementation in patients with diabetes or various forms of CVD have shown no benefit, and tended to suggest harm (1-5).
References
1: Tsai CH, Pan TL, Lee YS, Tai YK, Liu TZ. Evidence that high-dose L-arginine may be inappropriate for use by diabetic patients as a prophylactic blocker of methylglyoxal glycation. J Biomed Sci. 2004 Sep-Oct;11(5):692-6. PubMed PMID: 15316145.
2: Loscalzo J. Homocysteine trials--clear outcomes for complex reasons. N Engl J Med. 2006 Apr 13;354(15):1629-32. Epub 2006 Mar 12. PubMed PMID: 16531615.
3: Jahangir E, Vita JA, Handy D, Holbrook M, Palmisano J, Beal R, Loscalzo J, Eberhardt RT. The effect of L-arginine and creatine on vascular function and homocysteine metabolism. Vasc Med. 2009 Aug;14(3):239-48. PubMed PMID: 19651674; PubMed Central PMCID: PMC2840406.
4: Cosentino F, Hürlimann D, Delli Gatti C, Chenevard R, Blau N, Alp NJ, Channon KM, Eto M, Lerch P, Enseleit F, Ruschitzka F, Volpe M, Lüscher TF, Noll G. Chronic treatment with tetrahydrobiopterin reverses endothelial dysfunction and oxidative stress in hypercholesterolaemia. Heart. 2008 Apr;94(4):487-92. Epub 2007 Oct 4. PubMed PMID: 17916662.
5. Andrew M. Wilson, MBBS, PhD; Randall Harada, MD; Nandini Nair, MD, PhD; Naras Balasubramanian, PhD; John P. Cooke, MD, PhD
L-Arginine Supplementation in Peripheral Arterial Disease: No Benefit and Possible Harm
There is no evidence that carnosine inhibits AGE accumulation in vivo.
Food phenolics can inhibit the initial stages of glycation in vitro and in food systems, but they don't do so in vivo except maybe, maybe in severe diabetics.


I have some nigella sativa oil that I haven't gotten around to trying yet but it definitely seems promising based on the research. I have used a (counterfeit) bionase and another intranasal LLLt device, which I noticed nothing from. Maybe I didn't use it frequently enough to get results, but having a laser stuck up your nose for 15 minutes a day every day is less fun than it sounds.
I think the ginger and cordyceps are the most effective components of the stack, and the dosage for cordyceps is important IMO, considering the vast majority of clinical studies that achieved significance for respiratory health and exercise capacity were using somewhere in the region of ~3 grams.
I also drink a lot of sencha, I haven't seen much of anything to back it up, but I have a feeling that most types of catechins and egcg (and not just o-methylated catechins in benifuuki tea) have a favorable impact on allergies.
 As AjiPure, for reasons discussed under lysine, above.
As AjiPure, for reasons discussed under lysine, above.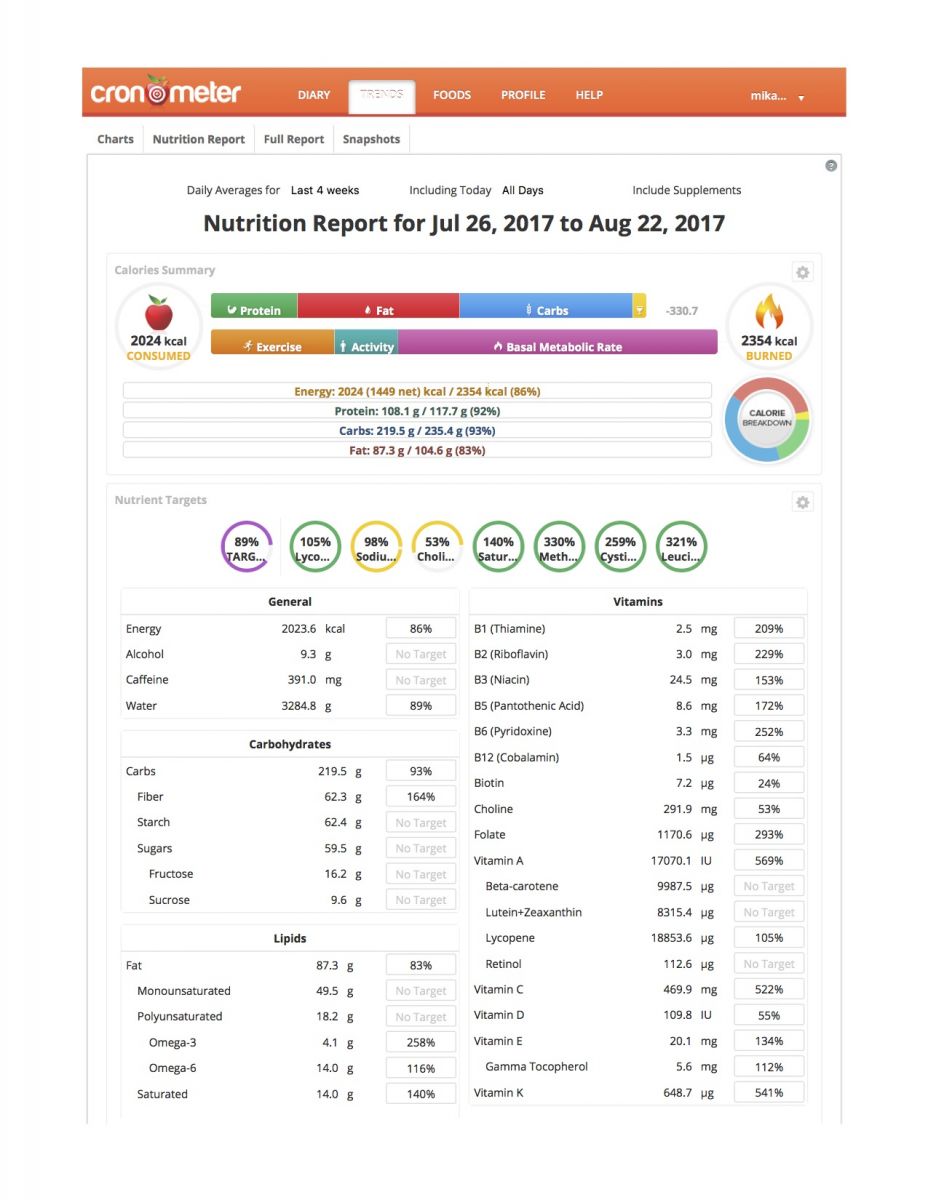


For me black cumin seed oil and guduchi extract brought great improvements with seasonal rhinitis too. Though I take each of the 5 you recommend (not all at that high doses all the times though), they didn't do much in my case. Ascorbic acid in high doses remains the go to remedy against symptoms, when everything else fails.
I'd add polypodium or it's extract; 20 hydroxyecdysone and black cumin seed oil.
This is the basic framework (exercise-capacity promoting portion) of a more complete stack that I take on a daily basis.
Additional supplements I take per day are:
Didn't rate, but you might consider grapeseed extract with the pterostilbene, as alone it can increase LDL cholesterol
Nice of you folks to rate this stack and then not give any feedback as to why you're rating it so low.
Do tryptophan benefits offset its side effects? I read this recently and decided it wasn't worth it: http://www.supplemen...de-effects.html
I suggest adding l-theanine instead.

If it were me I would take the curcumin, boswellia, and add ashwagandha and ginger to start with.
Vitamin D and fish oil yes if you don't spend a lot of time in the sun and eating oily fish.
I'd also eat a Paleo style diet without red meat, but plenty of wild seafood. This is important because breads and dairy, possibly nightshades as well could be contributing to the inflammation.
Have used the mentioned product , have tried others too.
I'm currently in the early stages of a multisystemic undiagnosed inflamatory disease, probably RA
I'm assuming I'm losing collagen as my nails are falling apart, have lines/pits in them and my skin is dry and has lost it's suppleness.
46/m
I haven't noticed any improvement
I also take UC-2
it's getting away from true anti-inflamatories but I suspect Ive gained an advantage from
UC-2 Undenatured Collagen 1 x at night empty stomach
CMO Cetyl Myristoleate 2x (3x/day)
Boron 10mg/Day
Mikey, the difference in our age. I'm 35, you're ~64. Collagen supplements are racemic. The "relative age" and health of the animal the gelatin comes from is important, especially as they age faster than we do, The average "relative age" of the animal is likely younger than 64, but may be older than 35. We also never know if the animal it's coming from is healthy or not, or if one bad animal spoiled the collagen supply. More research is necessary and pure specific collagens/elastins should be harvested from gmo bacterial sources and applied according to age and health condition. Otherwise, unless you're old, you're experience with collagen will be inconsistent and you could waste money on kilograms of collagen that is older than the stuff you're making.
The main stenosis as MRI gif (2009 - click to enlarge and rotate):

Psoriasis picture (don't click, if you can't see open wounds - 1996):
https://www.dropbox....mshala.jpg?dl=0
addendum (3rd July):
.. it was possible:
- first of all - to reverse a 60% walking disability from PAD
- ...
Only left to work on are CFS symptoms..
Meanwhile could get a 50% disability due to the CFS/ME symptoms again. Helps with yearly tax returns due to high health expenses.
For that reevaluation the investigating Neurologist ordered a brain MRI, which found an old stroke in the left cerebellum.

Therefore, one more potentially deathly condition not only survived, but not even mentioned its occurrence. ..thought it a miracle to have already outlived the 30% five-year mortality prediction from PAD, but now additional a much worse 50% one-year mortality with stroke!
- Chondroitin Sulfate - though not taken consistently as recommended here, after some months on about 5 g/d my intermittent symptoms from PAD completely ceased. And a 60% government-certified walking disability due to that has been revoked since!
When further analyzing which intakes have at least 30% increased during the 8 months before this substantial improvement - compared relative to my average intakes during these 9 years (leaving out Ayurvedics, since they all been added later and therefore all higher):
126% condroitin sulfate
117% paba
91% inositol
90% glutamine
85% medium chain triglicerides
82% magnesium sulfate
81% menaquinone-7
71% phyloquinone
59% rutin complex
59% kelp
55% cysteine
53% boswellia ext.
49% gingerols
44% tyrosine
44% lycopene
42% grape seed ext.
42% citrulline malate
41% lecithine
39% silica
39% pantothenic acid
39% milk thistle ext.
37% pomegranate ext.
37% methylfolate
36% potassium
36% copper (reduced after, since it caused to high than normal lab values)
35% silymarin
33% manganese
32% beta-carotene
31% punicalagins
30% trimethylglycine
30% ascorbic acid

I take 2+ (24+ grams) tablespoons of the Great Lakes hydrolyzed gelatin a day and yes, I have noticed a difference in my skin texture as well as my apparent ability to recover and the health of my connective tissues. These are subjective considerations, though. Just my thoughts.
With all due respect, I have a different opinion, Yolf.
Great Lakes appears to be transparent about the quality of their collagen, which is from grass-fed beef, which means that Great Lakes is aware of the inferiority of grain-fed beef products, in general.
Also, marbled steak is grain-fed, which means that it is inferior for purposes of longevity, as consumption of grain-fed beef is associated with an increased risk of cancer, cardiovascular disease and an increased risk of a shorter lifespan, as per a large Harvard study.
http://www.michaelmo...Meat_Kills.html
My current interest in hydrolyzed collagen comes because of a couple of years of highly "painful" parasthesia in my left hand caused by spinal stenosis and degenerated discs.
I had one of UCLA's best neurosurgeons recommend that I have a triple fusion in C-5-6+7.
I will not have a fusion.
I am attempting to do the 15th "medically impossible" thing that I have documented in re-aligning the misaligned vertebrae and regenerating the discs.
A 77-year old friend that has three degenerated lumbar discs reported that his "alternative" chiropractor recommended that he take the same Great Lakes Grass-Fed hydrolyzed collagen that you are asking about (two+ tablespoons a day), take 50 mg of manganese a day and use a Saunders traction device to pull the vertebrae/discs apart.
Within a year he reported that a new scan showed an approximate 80% improvement in disc height/volume.
I've been doing the same, except that I am seeing a doctor that has a traction unit that goes up to 35 pounds.
I report that the parasthesia in my left hand is about 10-20% as "painful" as it was about three years ago, so I am making progress.
I should note that back in the '90's Knox (gelatin) paid me a consulting fee in which I advised them to make the first hydrolyzed collagen product that eventually turned into the best-selling Knox NutraJoint.
Before that old-timers will remember that one had to dissolve gelatin in hot water to solubilize it. Hydrolyzing it breaks into tiny particles that dissolve in cold water, too. So, I have a history of studying this, although it was a long time ago and much research has taken place since then.
Published data show that hydrolyzed collage (gelatin) appears to preferentially go to collagenous tissues. This has been shown using 14C-labeled gelatin hydrolysate. https://www.ncbi.nlm...pubmed/11071580
One could hypothesize that humans are genetically adapted to ingest collagen via consumption of gelatin when eating animal tissues, and that a lack of regular ingestion of this raw material building block over a long period of time results in the loss or degradation of such tissues, in bones, connective tissue and skin (wrinkling). This notion is almost like thinking that collagen is a bit like an essential nutrient. If we don't get enough of it there is unnecessary, accelerated or premature aging caused by a deficiency.
Data show improvements in function for athletes - "Collagen hydrolysate is a nutritional supplement that has been shown to exert an
https://www.ncbi.nlm...ubmed/23949208/
https://www.ncbi.nlm...ubmed/21480801/
As to type l, ll and lll, I believe that there is merit in consuming sources of all three.
Also worth noting is that vitamin C is required for collagen formation, and a lifelong deficiency of vitamin C appears to predict more wrinkling of skin and loss of bone density. Most Americans only get about 300 mg of vitamin C a day.
One study looked at what we would get from a potential hunter-gatherer diet and found that such a diet would provide something around 2,300 mg of vitamin C a day. Is this more representative of what we are genetically-programmed to consume?
https://www.ncbi.nlm...cles/PMC283405/
If that is true, it could be one explanation for why the typical American is wrinkled and experiences a significant loss bone density as healthy bone is about 30% collagen and it is mostly collagen that gives bone its "flexibility," so that it absorbs impact without fracturing.
https://www.ncbi.nlm...pubmed/11149477
Best wishes!
I've seen better results with other stuff. The trick with collagen is the source. Beef Collagen is usually type I and III and can be sourced from aged cows who might be in worse shape than you as marbled steak is preferred and comes from older cows. It also contains alot of lysine which can harm your kidney's in the long term. There are definitely better options that will prove to be more consistent.

Thank you Adam, your advice is really welcome !
I've heard contrasting opinions on both bacopa and rhodiola. I thought that alpha gpc + 1 ingredient (like uridine, as you said) would be sufficient for my purpose.
Any opinion about dosage ?
Thanks again!
I am wary of huperzine, I think it would lead to downregulation of the cholinergic system, unless there is evidence to say otherwise. Galantamine would be a better option, but is often only available via prescription, and you'd only want to be taking a tiny amount if you lack relevant disease states.
I recommend checking out bacopa and rhodiola for a natural, mild cognitive boost.
Coffee would also be preferred over caffeine, as coffee contains beneficial phytonutrients in it that make it a health-promoting form of caffeine.
Seafood (even canned) would be preferred over omega 3s, as they contain health-promoting dipeptides and are more suredly health-promoting than fish oil.
Alpha GPC is a good choice, you might like to add Uridine as they are a good combo. Theanine is always good and cheap too.
Why would I want to use insulin spray in the morning? I imagine that just give me low blood sugar (perhaps deepen ketosis) and little to no other benefits.
Phenibut has been a life-changer for me - increasing sleep quality at night is much more important than making up for sleep-deficit related mood problems during the day. Sleep is fundamental, if you get it right, then you'll have phenibut-like effects throughout the day just naturally. I think many people with depression and anxiety have sleep issues, and fixing sleep can help reduce depression and anxiety. Have you tried taking phenibut for sleep? Most people haven't, in fact most people in the west don't even use it therapeutically, they'll tend to use it recreationally, which I think is really, really dumb (unsafe).
As of the date of this post, I have done many bouts of ketosis and fasting over the years, but I haven't done rapamycin yet. The logic behind adding rapamycin adjunct to the fast is to drastically increase autophagy in a small period of time. It's about time-efficiency, fasting and rapamycin each have side effects, and I'd rather get the side effects over and done with in a week rather than draw it out over the year with chronic rapamycin intake and regular bouts of fasting. There is also evidence that fasting really only effects autophagy effectively when sustained for many days in a row, as such, I assume regular, short fasts is not very useful for longevity, and the reviews on human fasting seem to agree.
There seems to be a fair bit of ANECDOTAL evidence that Lions Mane provides benefits with long term usage, though of course, some people dont seem to get any effects from it. I intend to take it for the next few months, thinking that it cant hurt, even if it does not do much for me.
As for the Noopept, up until recently I had been drinking too much for too long, though I have cut back significantly now. From what I have read, Noopept is good for repairing damage done by previous excessive alcohol consumption. From what I have read, both Noopept and Lions Mane both provide neurogenesis and other similar benefits, though I am not sure if there is any point in taking both, or if they both work on the same areas??? Any ideas?
I would love to eat more fish, but fish oil tablets are soo convenient. Not sure exactly what they do though.
Not sure how Lions Mane got in there, there isn't much evidence for how it works or what effects it has in humans.
I'm not a big fan of fish oil, doesn't seem to do much of anything, better to just eat more seafood.
I prefer piracetam over noopept, for everyday use. Noopept might be more appropriate in cases of brain trauma, but piracetam has a more thorough safety profile otherwise.
When I posted this comment, you hadn't filled out any dosages, so I can't comment on that.
Interesting. How about an an intranasal insulin spray in the morning? - along with eliminating the Phenibut at night - I think its a waste of its effects of enhancing sociability to use it at night. Much rather micro dose it during the day or cycle on and off.
>Each winter I plan to do a month of ketosis and a long (5 day+) fast with rapamycin adjunct
Have you actually done this? and whats the deal with rapamycin adjunct?
Cheers
i found out that anything lower that 30g of whey protein post-workout will give me a darned muscle soreness that keeps going for days.
Also, BCAAs help me a lot and i can definitely see an improvement.
I lift moderate weights but my training is very intense.
what about yours?
Also, it is important to know whether the type of cancer or infection is helped or hindered by antioxidant supplementation. Many cancers are made worse by antioxidant supplementation, so if the supplement doesn't have in vivo evidence for hindering the particular cancer then you should, conservatively, probably not take it.
I don't know how much evidence there is for these, but based on my priors about their magnitude of effect, I'd personally start with reishi, monolaurin and cat's claw.
You're already using reishi, one thing to think about is quality, there are lots of low quality reishi products, I get mine from nootropicsdepot.
Maybe do some more research on the other two and get back to us with a opinion/review?
Note #1: Yesterday evening i noticed nose bleeding: blood was pretty liquid and kept flowing for a while before clotting properly. I am reducing the gingko biloba intake from 120mg/day to 60 mg/day. Luckily enough I already posted the right dosage yesterday but... how will I change the stack ingredients next time?
I would supplement the nootropics gradually so that if something works you can know what it is.
Same thing for the research steroids you are planning to mix... triple steroid cocktail doesn't sound good to me... go step by step not all at once you're playing with your hearth, dick and balls, dude.
Plus i've always wondered why people supplements sulbutiamine AND multivitamins. Isn't sulbutiamine a vitamin itself? Isn't there the risk of hypervitaminosis?
They're not magic, but so long as it's within your price range, you can't go wrong with any of those compounds. I would imagine they extend healthspan, but probably not lifespan. Yet, healthspan is super important for quality of life
I'd consider replacing benfotiamine, iirc it reduces dopamine production. Instead, think about lowering blood sugar with thiamine HCl. Also think about switching to a fruit derived Vit C extract such as from acerola cherry. Don't forget to take ester C as well, they work better in combination.
What's the TMG for? Usually the doses are much higher. Like 1.5g/day. Riboflavin might be a nice cheap addition if you're trying to reduce homocysteine or preserve telomere lengths.

Forgot to add 1 gram each of carnosine and taurine, as well as 10 mg of PQQ, and 150 mg of benfotiamine.
Some details. I am a 67 year old male. Had an infarction at age 59, with 5 stents. Extensive atherosclerosis, high blood pressure, hypolipidemia.
My main concern 1) is reversing effects of cardiovascular damage (insofar as that may be possible), and 2) extending my healthy lifespan.
Just so you know, Namenda (memantine) is absolutely nothing like any of the compounds in that stack. Whether it's a smart drug is contended, but it definitely has some interesting effects that are useful in various particular medical contexts.
Nothing bad in that stack, though I personally wouldn't pair Galantamine and Huperzine together, that's a pretty low dose of Galantamine paired with a standard dose of Huperzine. I do think Vinpocetine is worthless, and that's a pointlessly low amount of Oxiracetam, but Aniracetam and Gastrodin might help with anxiety, and it seems anyone can benefit from Noopept and CDP-choline. I'd say give it a go and see.
So yeah, nothing wrong with Get Smart, just don't think of it as a replacement for Namenda.
I agree with dorho, i would also add a cold shower before bed, grounding on the earth if you can for 15 mins before bed. You can get an infrared bulb and shine that on your face for 15 min before bed too, seems to help calm my mind immensely. Are you taking magnesium or lithium orotate? essentials for sleep in my opinion. You can get UVEX blue light blocker orange glasses off of amazon for 10 bucks. Just wear them at night after the sun goes down when exposed to artificial lighting.
Cut back on the Beta Alanine, iirc, too much can cause tingling sensations and might not be good for nerves in your skin. Cut it back to 500mg. Too much glycine will make you tired... I think lower doses, like 2g and some ester C and regular C along with the quercetin you're already taking to retain the regular C longer is better than a ton of glycine... Same with taurine I don't see an appreciable difference between 1g and up to 4g. A nice CaMgZnCu and D3 supplement would do more for you than massive overdosing on any one thing. Synergy equates to better results imo, but it can complicate things. You should get the mineral complex already complexed... you can't measure accurately enough to make the ZnCu part safe unless you're making huge quantities of supplement mix.
Thanks!
I've been doing 16/8 for years now so that's good. I've been experimenting with 24-hr fasts, hoping to work up to a 2 days per week schedule.
What are the benefits of glycine and taurine?
I definitely have the resveratrol with fats already, either in the shake or in my food immediately after.
The reason for the budget is to make it feasible to keep taking them for many, many years. The higher the price the less likely I'll keep up with it.

I'd keep only the pterostilbene, use EMIQ (quercetine, with very high biodisponibility) 1 cap only every 10 to15 d (senolytics), add 10g glycine and maybe 3-5g taurine ed.
It's just me, but for your budget, you'll have to make choices...
Intermittent fasting can also be a good idea and costs nothing (16/8 is the easier way).
If you can keep resveratrol on the list, make sure to get it with whey or fat to improve absorption (coco oil/milk added to a whey shake would be nice)
Try sulbutiamine not daily, but up to three times a week, because of rapidly increasing tolerance, and higher dose, like 800mg - much better effect(I've tried up to 1.2g and I haven't noticed better effect above 1g.). You barely feel nothing after 10mg of noopept, at least 30mg - daily, I was taking mostly 2x30mg, sometimes 3x30mg, one dosage an hour before before exam/work. At 90mg(or 60mg If tired) taken in short term, you're starting to be a bit nervous,(aggresive?). Noopept has a short half-life period, something like 2-4hours(im not sure, but short). About PRL - its not cheap for me so to avoid building tolerance I was taken 5-10mg daily, or If I needed 20mg I wasnt taking it during weekends, and it works.

Check if you have high acetylcholine level, cause if it's the case, taking too much choline will cause depression.

The AOR Ortho sleep formula looks scary to me.
I've experienced all of them, only singly. Valerian, Passionflower, and Lemon Balm all have strong effects. The passionflower would make other things not break down as fast, lemon balm lowers thyroid. Overkill, with a strong likelihood of negative synergies

advise to remove tyrosine and taurine, reduce theanine to 1.5g, lecithin to 5g.
add lithium or ginkgo, NAC or ginseng, inositol or bacopa, and of course, green tea.
Unless you're a body builder or have an incredibly fast metabolism, you're better off with a more refined fish oil and a lower dose. Otherwise this is likely to lead to weight gain.
Way too much of some of this stuff? 3g of ALCAR? Tyrosine? Theanine? What is this for? Did you research max dosing levels for these?
I would eliminate Ritalin and everything, affecting glutamate receptors. In long term, it will only desensitize your receptors, leading to LTD or even be neurotoxic (prmoting beta amyloid - you don't wanna get Alzheimer's when you age, don't you?)
Eliminate the Ritalin (get more sleep?). And everything affecting glutamate receptors...in long term this desensitizes the receptors, some are going even in the way of affecting beta amyloids...
For me, Noopept worked much better than racetams. I was ordering it from PC. but find a stack with huperzine-A, alpha-GPC, phosphatidylserine and adaptogens (Examfit). It actually gives me a need for fork. I feel also increase in creativity, and I speak my mind with chicks (cold approach).
That information about Cinnamon is precious. I will eat more of it for sure (plus I love it) ! In yoghourt should be fine
EDIT : just ordered organic Ceylon cinnamon, and it taste so good. Ty Flex

what about something Glutamergic like Sytrinol or Cinnamon ? given it´s safe and doens´t fry Your brain over the time due to too much glutamate b/c noopept, racetams and NSI may or may not do this, I dont know.
because I have anyway a bad memory but it got even worse when smoking weed + Curcuma/Tumeric and I suppose that the anti-glutamergic effects are responsible for this.
btw look into this about cinnamon:
Cinnamon converts poor learning mice to good learners—implications for memory improvement
Hi Dorho. Thanks a lot for your feedback.
I agree with you for the liver. Sulbutiamine will be stopped at week 4.
Im not sure Noopept gives me a premium : 10mg sublingually isn't noticied. Not even 20mg. I guess my memory is improved however no special feeling at all.
This stack doesn't mean I doesn't eat well though. I was planning a fish oil intake, I'll do some research on dha+uridine+choline combo for sure.
About Berocca, it's funny I forgot to mention, I take 1 every week. However, despite having a LOT of vitamins (probably too much), the forms are not the most bioavailable on the market (often, the cheapest form is prefered).
I forgot to add RITALIN (40mg/day) in the aforementioned stack
MachineGhoastX,
I appreciate your feedback. I am going to cut down on Resveratrol and use a lower dose product once I am done with my current bottle. I am aware that PQQ is synergetic with Ubiquinol and adding PQQ is actually part of my plan.
Thanks,
Brighty

In my view, taking that version of resveratrol along with the pterostilbene is a waste of money. What's missing in synergy with the ubiquinol is shilajit and PQQ.
Since you're only mid-30's, you need to be careful you don't overstimulate yourself with any of this stuff, so be vigilant.
I take all of these together as I thought they are all synergetic with each other.
Brighty
I should also probably mention that I manage stress with mindfulness meditation and sticking to a healthy diet.
The cheap supplements that work for me are a quarter of a Berocca tablet (effervescent) and creatine. Sublingual methylcobalamin works nicely as well. The methylcobalamin sublinguals are usually so strong that a half or a quarter of a tablet is enough. Nicotine patch works as well although I'm not sure you want to go that route.
What I think is critical is eating healthily. Eating foods with high amounts of vitamins, micronutrients and phytonutrients really makes the most difference for me as far as cognitive functions are concerned: Broccoli, spinach, bell pepper, olive oil, mushrooms, beets, bilberries, almonds, chickpeas, fish eggs...
I'm myself also a former insomniac and former mirtazapine user and I also quit m cold turkey.
I've found that treating my insomnia naturally, without drugs or supplements, is the best and most effective way. I mainly utilize two pacemakers, blue light and coffee.
I make sure to avoid exposure to blue light in the few hours before going to bed. Blue light (coming from your computer's monitor for example) is picked up by intrinsically photosensitive retinal ganglion cells that turn it into a signal for the brain's circadian pacemaker, the suprachiasmatic nuclei in hypothalamus, effectively resetting your internal clock. I advise to avoid white LED lighting as it has a significant peak in blue wavelength and in case you use computer/smartphone/tablet/whathaveyou before going to bed, use a freeware application named f.lux which adjusts the RGB balance of your display according to the time of day.
This also works in reverse. If you don't get enough blue light exposure before noon (as is the case here in Nordic countries during winter), your internal clock is delayed, making you tired in the morning and wakeful during evening. I think this is the reason why coffee consumption is highest in Nordic countries.
Coming to the coffee topic, I use it as a pacemaker as well. I drink lots of coffee in the morning and that's it. If I drink coffee past noon, I often have trouble sleeping. I think I may be slow metabolizer of caffeine, although I'm not sure how that hypothesis agrees with my habit of drinking green tea in the afternoon without risking insomnia.
Choline Bitartrate seems to only be useful for curing a choline deficiency. It doesn't have any nootropic effects by it's self. Meanwhile, noopept is the racemic-like compound with, probably, the least amount of evidence (in English) as far as I'm aware.
If you're wanting legal acute effects, that really limits things, but I guess I'd go: caffeine, l-theanine, rhodiola, l-tyrosine and a [2-6]mg nicotine patch.
If you're happy to pay a bit, and just use occasionally, I'd add: oxiracetam, cdp-choline. Neither is 'cheap' but better than the noopept/bitartrate combo.
If you're just wanting things that *work* then: micro-lsd, selegiline, adderall xr, and a [2-6]mg nicotine patch.
Dextromethorphan - 15mg twice daily with magnesium 500mg (tid) seems to work the best for me.
drusko, are you serious? Isn't DXM absolutely terrible for your brain? I was addicted to DXM in high school and I wasn't able to remember words like "tree" or "car" (albeit I was taking much larger doses, closer to 400-1000 mg). I know there are stories about DXM deadening areas of the brain, essentially turning them into grey matter, although I think this claim MAY have been discredited.
What research do you have that proves micro-doses of DXM are not harmful? Is there any risk of addiction or "desiring" to take more?
Simple and decent.
I am hesitant to say, but I don't think piracetam improves memory or performance unless you're already have a deficit, I tend towards lower dosages too, just as a neuroprotectant.
Noopept lacks human trails, but I also would predict noopept is at worst harmless, and at best slightly enhancing. You could take it in the morning at at lunch if need be, and I'm not aware of any contraindications with your listed nootropics.
I prefer armodafinil over adrafinil, and drink a few cups of green tea which gives me theanine. You could take theanine any day you wanted to, only cost would be a factor.
Would you suggest some of the other racetams for memory? I just wanted to start with piracetam, use it consistently, and see if I notice any improvement, if its only very negligible, I might move on to ani/oxi/phenyl, any advice on cycling with noopept?
also had pretty bad sleep last night using theanine before bed, so that was weird
Simple and decent.
I am hesitant to say, but I don't think piracetam improves memory or performance unless you're already have a deficit, I tend towards lower dosages too, just as a neuroprotectant.
Noopept lacks human trails, but I also would predict noopept is at worst harmless, and at best slightly enhancing. You could take it in the morning at at lunch if need be, and I'm not aware of any contraindications with your listed nootropics.
I prefer armodafinil over adrafinil, and drink a few cups of green tea which gives me theanine. You could take theanine any day you wanted to, only cost would be a factor.

You said you take fish oil with these as they are all fat soluble. Are you sure they are all fat soluble??
Has anyone here tried Visoluten? It is a peptide for eye health or improved vision.
I like the stack a very reasonable, responsible plan. I would agree that ALCAR is not necessary. It may also contribute to heart problems down the road and it makes me personally more robotic, anti-creative.
I would rebuild the plan. I'd start with taking caffeine only for three days, then add the next thing on top for three and so on. This way you'll find out what's causing the headaches and nausea, and throw it in the trash, if you find out. You also can't take Phenyl every day. It builds a tolerance quickly.
I would cycle the racetams, especially Phenylpiracetam, it WILL lose it's efficency. Noopept is supposed to be cycled. You could go three days PP, four days Prami. On top two weeks Noo, one week Ani. This way you will also learn much more about the individual racetams.
seems like this sub is pretty dead since the restructuration/relocation..
Oxi is a good choice, L-tyrosine can't hurt, I wouldn't touch 5-HTP for various reasons, I prefer Bacopa over Lions because there's more evidence of it's efficacy in humans.
Uridine is a good choice, but I am not sure, do you need both uridine and Alpha GPC? You could get the benefits of both by taking CDP choline instead, as it converts partially to uridine.
B12 is good, go for the methyl form, but I am not sure why you'd want B1... perhaps makes more sense to take methylfolate?
Make sure your mag and zinc are high quality, I tend to go for the chelated forms (glycinate or something like that), and don't overdo the zinc (there is such thing as too much!)
Some people speak very highly of Ginkgo, but I think it's relatively worthless.
I hope that helps! Good luck, and remember being productive is more than just nootrpics. Use Google Calendar and HabitRPG to get your life organized. Keep track of your short term goals, break up tasks into subtasks. Sleep enough! Surround yourself with people more intelligent than you, and be passionate.
neurodegenerative disease not disorder* sorry typo, and cant seem to find an edit button.
additionally I forgot to mention that I plan to add CDP choline as a choline source soon.
so far I simply consumed roughly 2 eggs every 1-2 days
I take Citricoline on some days when I don't work out and GPC when I do and some others. Citri/CDP coline can make me kind of tense sometimes.
Its a half a 150mg Armodafinil. But in any case I don't feel like I need it every day and I don't want to build a tolerance.
I generally sleep fairly well, always have. If anything I am in the best shape of my life. My girlfriend does wake me up in the morning when she goes to work and then I have to go back to bed. But I feel well rested. Sometimes I will take 5-HTP and/or CBD oil to help me sleep. For getting to sleep, I highly suggest CBD oil. It is legal in all 50 states. Cibdex seems to be a reputable brand which works well for me.
I have heard that on paper NALT seems less useful then L-Tyrosine but that in fact many anecdotally find it to be more effective.
I have not gotten my D levels checked. I do go outside more then most Americans, but that may not be saying much.
I do appreciate the feedback, even if it seems like I have been a bit challenging to what you say. I just like to have all the info out there.
I'm no doctor, but I'd think it's pretty safe to take a quarter daffy any/every day, if you feel you benefit from that. That could help with focus when reading, and also help reduce your appetite (to help lose weight). However if you plan a creative session, anecdotally it's not good for that.
NALT seems safe, and if it helps with your depression then that's a good thing. I should try l-tyrosine myself, but I won't be using NALT.
Examine says: "N-Acetyl-L-Tyrosine appears to be able to contribute free L-Tyrosine in vivo after administration IV administration, but only able to increase L-Tyrosine concentrated 20% despite much larger increases in serum NALT. 56% of the adminstered dose of NALT is excreted in 4 hours and another study suggests that, overall, 35% of the total NALT dose (administered parentally) is excreted via the urine as NALT and not L-Tyrosine." So NALT is not worthless, but may not play the same role as l-tyrosine because it's excreted before it's converted?
As for ALCAR, lots of people will disagree with me here but I don't think it's anything special (except, maybe, for vegans).
Assuming you don't strictly follow a diet, adding DHA is probably a good idea. Looking over the tables at examine.com I prefer CDP choline over GPC, but that might just be a personal preference.
If the cost of the stack is a strain, I think the evidence for glucosamine is weak, so maybe drop that?
Recommendations: people with atypical mood and/or are overweight often sleep poorly, or follow bad sleeping habits, melatonin can help with this. Both selegiline and tianeptine comes highly recommended for hedonic modulation, I have had success with these compounds, but I am looking to replace the tianeptine with some thing else because it can be hard on the liver for some. I'll be trying a combo of ashwagandha and micro-lsd in the near future.
Have you ever had your vitamin d levels checked? There is a high probability that you have low vitamin D, but that isn't to say I know you *do* have low vitamin D, just get it checked.

and you may be interested in adding a good ashwagandha extract to augment your strength training. ksm-66 is pretty cheap on amazon - Examining the effect of Withania somnifera supplementation on muscle strength and recovery: a randomized controlled trial
avoid vitamin c (and possibly fish oil) around the time of your workouts - Oral administration of vitamin C decreases muscle mitochondrial biogenesis and hampers training-induced adaptations in endurance performance
If it hasn't been mentioned, I'd take methyl folate if you haven't been genotyped. Too much can lead to problems, and lower amounts might be problematic in some populations.
Unless enteric coated, I would take the CoQ10 and maybe the PQQ away from any of the acids or with alkaline conjugated supplements to improve absorption.
Grape seed ext. should be taken every other day, not sure about your dosing, how old are you?
Should I cycle any of these or is this solid for long term use?
Thanks for your input and analysis, it's reassuring. I was thinking about food with carnosine but read contradictory things for and against and just took a stab.
Take Carnosine on an empty stomach.
I don't really see any specific blood pressure lowering supplements. You would want something like hawthorne berry standardized to vitexin for that. Grapeseed extract does increase NO though.
You ideally want to use ubiquinol instead of CoQ10 (ubiqinone). The bioavailability is several times higher; further enhanced by shilajit. If 50mg (equivalent to at least 400mg CoQ10) once a day is too strong for you (i.e. insomina), then I guess CoQ10 would work, just make sure you get an enhanced absorption product such as Q-Gel.
If you want to use specifically tumeric instead of standardized curcumin extract, then make sure you use a SuperCritical CO2 extract to get a full spectrum of phytoactives. If not, then you need to decide if you want curcumin for general anti-inflammatory support via curcuminoids or corssing the blood-brain-barrier with intact free curcumin (useful for getting rid of the Alzheimer plaques and chelating iron).
And of course, you want to use natural folate or methylfolate, not synthetic folic acid.
Take Carnosine on an empty stomach.
I don't really see any specific blood pressure lowering supplements. You would want something like hawthorne berry standardized to vitexin for that. Grapeseed extract does increase NO though.
You ideally want to use ubiquinol instead of CoQ10 (ubiqinone). The bioavailability is several times higher; further enhanced by shilajit. If 50mg (equivalent to at least 400mg CoQ10) once a day is too strong for you (i.e. insomina), then I guess CoQ10 would work, just make sure you get an enhanced absorption product such as Q-Gel.
If you want to use specifically tumeric instead of standardized curcumin extract, then make sure you use a SuperCritical CO2 extract to get a full spectrum of phytoactives. If not, then you need to decide if you want curcumin for general anti-inflammatory support via curcuminoids or corssing the blood-brain-barrier with intact free curcumin (useful for getting rid of the Alzheimer plaques and chelating iron).
And of course, you want to use natural folate or methylfolate, not synthetic folic acid.

Nice, thanks for sharing, LiveWell! I like green tea for that as well, matcha especially. I'm not sure that it would mix very well with other drinks but the powder on its own goes great in a smoothie. I've had mixed results with caffeine + L-Theanine also (which is the active ingredient responsible for increased cognitive function and stress-reduction in green tea). Probably best to stick to the real thing if you can. Matcha is soooo good.

I always drink a strong cup of Green Tea (cold steeped to avoid bitterness) before a workout. The caffeine content isn't overly high but the green tea has a way of increasing fat oxidation.
I add it to my ZipFizz (usually the Orange Soda flavor) for more caffeine + vitamins.
Background: Current interest in the role of functional foods in weight control has focused on plant ingredients capable of interfering with the sympathoadrenal system.
Objective: We investigated whether a green tea extract, by virtue of its high content of caffeine and catechin polyphenols, could increase 24-h energy expenditure (EE) and fat oxidation in humans.
Design: Twenty-four–hour EE, the respiratory quotient (RQ), and the urinary excretion of nitrogen and catecholamines were measured in a respiratory chamber in 10 healthy men. On 3 separate occasions, subjects were randomly assigned among 3 treatments: green tea extract (50 mg caffeine and 90 mg epigallocatechin gallate), caffeine (50 mg), and placebo, which they ingested at breakfast, lunch, and dinner.
Results: Relative to placebo, treatment with the green tea extract resulted in a significant increase in 24-h EE (4%; P < 0.01) and a significant decrease in 24-h RQ (from 0.88 to 0.85; P < 0.001) without any change in urinary nitrogen. Twenty-four–hour urinary norepinephrine excretion was higher during treatment with the green tea extract than with the placebo (40%, P < 0.05). Treatment with caffeine in amounts equivalent to those found in the green tea extract had no effect on EE and RQ nor on urinary nitrogen or catecholamines.
Conclusions: Green tea has thermogenic properties and promotes fat oxidation beyond that explained by its caffeine content per se. The green tea extract may play a role in the control of body composition via sympathetic activation of thermogenesis, fat oxidation, or both.
Oh and I'll add that Ephedrine is legal to purchase where I live in Canada as a nasal decongestant. It is NOT legal in the USA as far as I know. I'm not sure about other countries.
The recommended dose is 8mg 1-4 times daily (no more than 1 tablet per dose). This dosage is likely precautionary because of all the reported side effects and legal stigma. I have bad allergies and have used it while sick. It does indeed work very well as a decongestant but I find that I need at least 16mg to really get some relief. But that may be due to tolerance.
I've had good results by adding caffeine to this stack but not too much! Maybe a cup or two of coffee but that's it. You can also substitute the aspirin for a fish oil supplement too if you're afraid of any negative side effects.
Be warned that this stack can be addictive and tolerance develops quickly.
Interesting. I have never heard of any of these but I'm relatively new to nootropics so no big surprise there. Good results so far?
Comments & Observations
Results
After trying this stack for a couple of days now, I'm less than impressed. One thing is for certain: it definitely increased my attention span but unfortunately at the cost of a constant, mild headache and a bit of nausea. Perhaps I'm not taking enough choline? I also did not notice any increase in mental or physical energy. There seems to also be some brain fog but I'm not sure if it's that or tunnel vision from being so focused.
On a positive note, the anti-anxiety/anti-stress properties seem to be somewhat effective. I had a pretty rough day but managed to keep my emotions and stress level in check. I would probably attribute that to the L-Theanine but it's difficult to say for sure. My overall thought process, memory and communication skills seem to have improved slightly. I didn't get much sleep last night but I was still able to function rather well today and I didn't really "feel" tired at all.
All in all, if I had to rate this stack based on my experience so far I would give it a 5 or 6 out of 10 for effectiveness. It's not quite what I'm looking for but there are definitely some elements of it that I'm interested in pursuing. It's not something you want to take if energy is what you're after but if you want long periods of focus for studying or coding, give it a try. To me the headache is not worth it even though it's not that bad. I probably need to tweak the dosage/frequency or substitute some of the ingredients.
On to greener pastures!
Cheers.
Edits: Correct typos and add final thoughts.
Could improve the layout of this regime by including ALL your regular intakes in the Regime [Ingredient] table. That way, for those ingredients, they need no further explanation in the description, cutting down on text.
Just personally, I prefer well reduced stacks. This seems to be a kitchen sink regime, yet lacks any really powerful substances. One issue I take with having lots of herbal supplements is that such products are notorious for either having no active ingredients in them at all, or being full of heavy metals or other pollutants, thus 1) I try to be selective with herbals and 2) focus on sourcing the materials fresh, raw, regulated food grade, rather than buying unregulated prepackaged stuff.
How does it work for you? Give us a before and after comparison, perhaps? Have you tried eliminating each item one at a time to see if there are any dead weight supplements?
I am unsure whether you should do this stack for two reasons.
Firstly I just don't think the pay-off is equal to the costs incurred for most amino supplements in most contexts, specifically if you're eating a decent amount of protein.
Secondly, methionine *restriction* seems to be a very legitimate longevity strategy and even explains part of the effects of calorie restriction. I saw one study that suggested adding high protein to a calorie restricted diet no longer confers the benefits of calorie restriction, which is why people started talking about protein restriction as a form of life extension... it turns out protein isn't so generalizable, but methionine is likely the bad guy. Do a few weeks of research yourself and then tell me if you agree with me or not.
[Deleted post integrated into Regime Description]
Also, if you're not going to give it 5 stars, please comment below and suggest what could improve it.
whoops, I need to recalculate the totals, for some like copper I just realized the data was providing miligrams (mg) even though the total was based upon micrograms (mcg). I also put the vitamin C from orange juice into the wrong food group which I didn't copy down for my daily diet. So I am getting enough Copper and Vitamin C and they shouldn't be supplemented.
Calorie estimation of the above diet is about 1,960 calories. A sedentary, 6FT tall 30yr old male needs 2,096 calories to maintain his weight. So it's pretty close. 136 calories of oil, seasoning, flavoring or calories without any additional amino acid is very easily plausible. Slightly larger or smaller portions than the estimates it is also plausible If the portions are larger by that much it probably won't make a significant difference in the dosages.

Yes, NMDA antagonists do seem to be the best combatants against OCD. Dextromethorphan - 15mg twice daily with magnesium 500mg (tid) seems to work the best for me.

If you'd like to taper faster, you can begin at 2mg (or maybe 4mg), then double every 4 days.

http://www.lef.org says that uridine monophophate has cognition enhancing capabilities
Uridine-5'-monophosphate (UMP)is a compound naturally found in the milk of nursing mothers and is essential to humans when brains are the youngest. Uridine-5'-monophosphate also supports superior cognitive function in aging adults.
perhaps the monophosphate versionof the uridine described at Zybez list would be even more beneficial
Looks like a pretty good stack.
The gotu kola dosage may be a concern.
Evidence has shown that excessive dosages of gotu kola may cause stomach pains and dizziness.
isn't there a compound called thymosin that works on the thymus that seem to have gotten lost and forgotten due to FDA regulations etc.
But I think this product here is the same product as thymosin only called thymucin:
https://www.pureform...erapeutics.html
I would appreciate if someone here could explain what the importance of the thymus is, I'm a bit clueless about it due to its obscurity. I think thymosin was considered an immune system "stimulant". I'll find the source of where I read about it once I have time. Chime in everyone...
You can also replace Semax with N-Acetyl Selank (300mcg once per day) for a more direct anti-anxiety effect.
I was wondering if someone could help me with my stack. It is working for the most part but in the afternoon I am finding myself yawning very loudly. I don't want to take more smart caffeine because it seems like it would be over doing it. I am going to try b12 and a multi vitamin. I am thinking that something might be medically wrong because this is a lot of supplements.
BTW. I have Zoloft which i stopped taking about two weeks ago so I can properly test this stack. but i took this stack with the Zoloft for one week and everything was great. I did taper off the Zoloft so withdrawal is not the issue.
Is there anyway to delete or edit a stack? Also, I've typed out my 15 ingredient stack and when I hit add stack it just deletes everything.. :(
Sorry for the clutter..

I don't get it: you said 30mg of 'piracetam hydrazide' and NSI-189; but what's indivdual dosage of these? Isn't it phenylpiracetam hydrazide u mean btw? I'm interested to discover how you got on with mixing tianeptine with NSI-189?
Alpha GPC dosage:
Piracetam 1:8= 2000mg / 8 =250mg
Noopept 1:20 = 10mg x 20 = 200mg
This would make a total of 450mg x 3 = 1350mg per day.
This seems too high for me, and taking it after 1300 may cause problems with sleep later on (from what i have read).
At the moment i am taking the dose of 400mg alpha gpc, once in the morning and once a lunchtime. I will see how this goes.
Omega 3 - Boots 1300mg capsules containing the following: Eicosapentaenoic Acid (EPA) 95 mg & Docosahexaenoic Acid (DHA) 250 mg
Lots of discussions on the forums of the benefits of EPA vs DHA and ratios.
Tied not using any Alpha GPC today, 2 hours after i got a headache. So took 400mg of Alpha GPC, headache gone, mind feels nicely oiled. Funny expression but describes perfectly the feeling.
Went well today, in fact felt great most of the day. Think i may have been over doing it with the chlorine gpc, time will tell. More tuning required :-)
Still playing with the alpha gpc dosage, today dropping to 400mg to see tomorrow may not include it, depending on today.
Too much Noopept. Personally I find even 5mg builds up and becomes too much very quickly, the perfect dose is almost too small to measure. When people say they don't experience anything with nootropics, it's usually because they've overshot the sweet spot. Almost every post I read on here involves taking far too much of everything!

I would take the noopept sublingually (so that none of its is wasted - more potency and also so it works more rapidly)
- as well, I would only take the noopept in 10 - 15mg increments (i'm not sure if daily means each dose or within a day)
The piracetam is dosed pretty high. My max daily dose of piracetam is 1400mg and even at that dose, I have experienced tension in my neck and irritability.
(Just an fyi, if you do have these negative symptoms, you can go buy some liquid magnesium and it'll solve your problems)
Your alpha GPC seems a bit low - if I had it that low, I would feel brain fog and headaches all the time. We're definitely all different, but if you feel tired for no reason, or headaches - I would most certainly raise your amount (I take 450mg w/ each dose)
I used to take spirulina but it actually leads to deficiencies in B12 because it gives you a type of B12 that doesn't work for humans, and in doing so, binds to the places that the other B12 taken in by other food would normally bind to (leading to their excretion instead of their absorption)
On the cod liver oil - Nice choice!!! I hope you're using a cold-pressed kind w/o any kind of fortification (because that would mean that the oil has been sucked dry of its nutrients and is now being replaced w/ lesser nutrients)
All in all, nice stack. The piracetam and noopept really work wonders!
to start with digging in scientific background information, please take a look at:
If anything will help with anti-aging its that stack right there. Maybe low dose TRT as well.
You also might also want to check out TB-500 and perhaps some type of growth hormone releasing peptide to stack on top of your 2-4 IU's. It could potentially make it more like 6-8 IU's. And Growth is pretty expensive so it might be something good to look into.
Havent heard of Ta-65 before. Looks interesting! Thanks!
Interesting. What was your Free T?
I've tried all of the various T-boosting herbs and haven't been impressed -- either they do nothing at all or quickly induce negative feedback, even when rotated weekly. I'm currently using DIM (anti-aromatization) and Nettle Root (anti-SHBG) along with topical DHEA. It works minorly.
Why did you go with Aromasin instead of Arimedex?

Jeff McJackoff is an obvious troll, who uses some stereotypical mostachio creepy mexican picture as an AVI; a select choice for trolls? Then there's the "McJackoff" name, clearly fake..in my experience, people who use a first and last name, especially common first names or coupled with fake last names, ESPECIALLY with the"Mc" or "Mac" prefix - are commonly trolls or just plain idiots; this idiot is no exception.
Jeff McCrackhead, please go fuck yourself with a mutated toxic toad.
I cut out the Ashwagandha, Garlic, and Fish Oil. Replacing Fish Oil with Krill Oil. Now taking Turmeric and (Echinacea, Astragalus and Reishi) only occasionally. I intend to eventually take carnosine and coq10.

I've not found any issues with antisocial thoughts/behavior (beyond baseline) with the L-Theanine. However, I have to admit I only have it as part of a stack that includes occasional Piracetam, which I find to be very positive in terms of interpersonal interactions.
Thanks protoject. I've confirmed your statement - my mom had some .3mg Melatonin that I swiped from her, and it seemed to be effective even though I've been used to taking the 10mg caps five days a week.
To update you all, I've found the Noopept has more or less seemed to plateaued in terms of noticeable, day-to-day interval changes. The greatest changes were in the first 1-2 weeks. I intend to travel out of the country for two weeks this coming Monday, so I will stop using my stack at that time - I'd rather not have to try and explain what Noopept is and why I use it to nosy border agents. I'll try to take note of the withdrawal effects, if any, though it will be difficult to distinguish, as I will be suffering from some pretty severe jet-lag as well.
I've only been trying to use 1.5-3 g of Piracetam perhaps 2-3 days a week to avoid tolerance and brain fog. Honestly, 3 grams with all of the other things is a bit much - I sometimes feel overwhelmed by the flood of thoughts and the overall sensory input, though I'd reason that I can read about 300-400 words per minute, with my normal being only 100-200 when focusing normally. (It has essentially zero impact on my typing speed, lol) The Piracetam also continues to have a beneficial impact on my mood even at 1.5 grams.
Of late, I've been doing more research on Noopept. While some studies seem to paint a very rosy picture of its safety profile (1), I was a little surprised by one of its mechanisms, namely the effect of increasing Nerve Growth Factor (NGF). This protein is surprisingly very important in a number of cells throughout the body. Importantly, it works on neurons to promote growth (who'd have guessed?) and prevent apoptosis. However, it doesn't simply have this effect on neurons; in fact, it has a surprising impact on cancer cells! (2) This includes but is not limited to: melanoma, breast cancer, and prostate cancer. (3) NGF works to prevent apoptosis and encourage growth. This is particularly worrisome, as we all have at least some small number of cancer cells in our bodies, which our immune system naturally destroys.
My question now is this: does Noopept encourage NGF to be generated in all tissues throughout the body, or only in the nervous system? If it is effective outside of the nervous system, this could be quite worrisome, as it would essentially increase the risk of all major cancers over a long period of time. I can't imagine I'm the only person to consider this unfortunate possibility.
One other good note is that the substance seems to have anti-inflammatory/anti-oxidative effects. (4) This may counterbalance any potential cancer inducing effects, but I don't know if I feel safe assuming this going forward.
1) http://www.ncbi.nlm....ubmed/12025790
2) http://www.sciencedi...212492614000621

only 0.3 mg melatonin is required in humans to acheive the desired physiological effect. (can be achieved using liquid melatonin supplements)
If that doesn't hit the spot you could always try between 1 and 3 mg, 10 seems a bit high for daily purposes.

It seems like a good stack, but what about prolactin? Mucuna pruriens or perhaps a phytoSARM would make this beautiful!
Acetyl-L-Carnitine would be a good add too!
Haha, ok. I bought a great blend of Matcha and will try that recipe tomorrow. If I run around with a yellow face all day long, I will find you I still have to find a way to handle that nasty coloured stuff. Usually, I add it to a bowl of rice. Putting it in capsules is a pain, so I ended up making a paste which is much easier to deal with: http://drarjan.com/t...te-golden-milk/
Taste is not that amazing :D But it is not as bad as I thought it would be. You can add stevia to sweeten it a bit.
Sounds like an very interesting cup of tea. My question: how does it taste?

I am curious about armodafinil. Would you say that it is helping you have more energy and alertness on a constant basis?

Hello,
Hi Dan,
I'm looking for a stack aimed at preventing macular degeneration, do you think this would fit?
Right now I'm just taking Goji berry extract as I'm pretty young (36) but both sides of my family has the problem, so I'd like to be preventative.
Thanks,
MB
I think this would be a good fit for preventing macular degeneration.
I recommend you to look up the AREDS I and II studies.
Also, here is a good source of info regarding eye problems: http://www.reviewofophthalmology.com/
I have tried Coluracetam. The effects on my eyes are very good. The visual fatigue practically disappears.
I'm making Coluracetam a permanent part of my stack.
The dosages I tried are:
- 100 mg 3 times a day (which I consider megadosing)
- 80 mg 3 times a day (as recommended in the clinical studies for major depressive disorder)
- 20 mg 2 times a day (as recommended by Ceretropic)
I prefer the lowest dosage (the higher one is a bit too much for me).


Hey are you still taking this stack? I decided i'll give it a try minus the caffeine and see if it helps me with the numerous buisness-related tasks as well as some reading I need to get done. I suffer from adhd-type symptoms, anxiety and various motor ticks so I might have to drop the optionals if they increase the prevalence of ticks or increase anxiety. Is this safe for long-term brain health? Withdrawal symptoms? Thanks.

why did you ditch the coluracetam? What are your thoughts on sublingual NSI? (why not?)
I wanted to try something different but I have an understanding on the effects of both and feel that Coluracetam is best, but stacked with some Choline source. Sublingual NSI is by far the best anti-depressive agent I have so far. CBD is pretty good as well.

why did you ditch the coluracetam? What are your thoughts on sublingual NSI? (why not?)

How does this works for you? Is L tartrate carnitine better than ALCAR in preventing ache upregulation? Where do you base this on? Thanks
how are things going, have effects remained constant over time ? could you pls. write more about your current progress with this combination ?

Greetings, would you be able to recommend the most useful in your opinion, or most noticeable in potency and/or effect(s) to me from your current list/stack? It would be most appreciated. Thank you for your time.
Sincerely,
Jacob A. Eder;.
That's highly impressive, and incredibly complex, well done - I hope one day to see your name in pharmacies across the world.
I think the general rule for racetams is that they all affect people differently. And I'm pretty sure people have said to cease taking racetams if you experience any lasting side effects (effects lasting 2-3 days or something). Also I feel that some of them took an excess for their first time, which caused negative results. I can say myself that I took 2.4g of piracetam at first and had a terrible headache, cut it down to 1g, everything was much better. There is an n shaped dose response curve for racetams, after all.
It also doesn't make sense that some of them took it for 3 weeks and experienced chronic headaches... I mean, wouldn't you stop after having the first or second headache? Why push it to 3 weeks?
Plus, it's not like piracetam is the only nootropic out there, people can always switch to herbal nootropics or a different class of compounds altogether.

Hi Dan,
I'm looking for a stack aimed at preventing macular degeneration, do you think this would fit?
Right now I'm just taking Goji berry extract as I'm pretty young (36) but both sides of my family has the problem, so I'd like to be preventative.
Thanks,
MB
Cant answer You that question, it seems problematic.
You could try :
- Rhodiola Rosea because it increases Dopamine via ( reversible) mao inhibition.
- egcg ( green tea polyphenols) because it releases glutamate and increases Shh( sonic hedgehog) in the Hippocampus
Keep in mind that this is a potent bloodthinner via reducing platelet count, among others
See this very informative site:
http://www.raysahelian.com/egcg.html
http://www.raysaheli...m/greentea.html
- Clausenamide, from Clausena lansium, could be a herbal alternative
http://www.longecity...rbal-piracetam/
- Hupericine
Not sure whether its a everyday thing, I would rather cycle it and dont take any choline with it !
Because due possible chances of enduring cholinergic overactivation ( just my theory)
See: tabun/sarin/mustard-gas poisioning
I dont have much experience with them in regards of learning.
So its just hypothetical, because dopamine and glutamate are also implicated in learning.
Actually I just wanted to thank You for this very informative site,
but I guess the best thank would be by giving You those hints/suggestions ;-)
Hope they are actually helpful though ^^
I have read many times that L-theanine was a bit anti-social ? What is your opinion about that ?
I haven't heard anything about that at all. However, I have ditched most of this list now that I have tried other stuff. Wish you could edit and/or delete these stacks!
I highly recommend trying out Chaos and Pains Da vinci with some NSI-189 and Piracetam. It pretty much has the Picamilon inside it, with a load of other goodies for promoting mood!
I think tonight I'm going to try going up on dosage by 250mg on each one. ...
Move from
1gm of Piracetam to 1.250 of Piracetam twice a day ( afternoon/night time)
250mg of Aniracetam to 500mg of Aniracetam twice a day. (afternoon / night time)
I will add choline to this stack at 250mg of it twice a day (Afternoon / night time)
What do you guys think about this dosage?
I have read many times that L-theanine was a bit anti-social ? What is your opinion about that ?
Any feedback on this? I thought someone would be able to answer my question...
Ok... should I be worried? Just read this article on the dangers of racetams, and it seems like a lot of people have had bad experiences?!
http://selfhacked.co...with-piracetam/
Sounds like a good idea, but how do you do a blind-test on yourself with a placebo?
Easy: Just put a sugar pill that seems like any of the ingredients and mark it with lets say a dot made with a fork or a knife. Eat it, and then at the end of the day look for that pill. If it is not there then you ate it, and if you felt anything then it was only placebo.
Did you figure out what was causing the muscle twitching?
Without using the (optionals), muscle twitching is almost nonexistent. I usually experienced that when using too much caffeine because it synergized too well. The feeling is pretty close to coffee jitters and moderate doses of adderall so I recognized that it was most likely the caffeine.
Noopept seems to be the cause the minor emotional blunting so cycling may be needed (depending on the person).
Also, caffeine is extremely bitter so taste is significantly altered when I add 250+mg to a standard vitamin water... using standard 200mg caffeine pills is a good taste alternative (however you sacrifice the convenience of gradual consumption)
How did you get your hands on NSI-189....? It's in R&D for DARPA/Central Research Agencies.
You must be top secret. :D
Nope, you can get it online if you look around. TeamTLR is a good place to look!
How did you get your hands on NSI-189....? It's in R&D for DARPA/Central Research Agencies.
You must be top secret. :D
Phase these in one at a time over the span of many weeks (at least 10 days per; and, if you really want to work toward a good stack, do a separate blind-test on yourself with a placebo for each noot that you phase in).
Jumping into any stack is a mistake. You won't know where the positive, and more importantly, where any adverse side effects are coming from, with any degree of "certainty" at least.
How do I edit this damn thing? I need to re-link the data for my supplements.
Here they are anyway:
http://www.aor.ca/pr...ced/ortho-core/
http://www.aor.ca/pr...ta-resveratrol/
I can't live without my coffee The L-Theanine seems to counter effect any anxiety I might normally get from taking too much caffeine. Combine that with Aniracetam, and I have no trouble having a conversation with a complete stranger. I've since added 10mg of Noopept twice a day.
No Objections.
As discussed before, try to minimize amount of iron and copper from a multivitamin.

Great! I'll think I'll add this to my list of things to try. Phenibut as a lot of us know is a tricky substance when not properly dealt with. I also just recently posted a stack on here as well that was suggested by someone else, which also included ingesting Phenibut daily. I've found though that I wasn't able to handle the side effects of a low dosage for even just a few days, so now I'm gonna start over soon when I buy the free amino acid version of it. What do you suggest cycling Phenibut with once tolerance is seen?
Well to be honest I have stuck with this dose and have cycled it so I don't become dependent on it. In addition, effects are more pronounced if you cycle it as you don't become tolerant to it. Not worth taking it "every day" as such as you will just become dependent on it and will suffer withdrawals. Only use once to three times a week max. :-)
If you have tolerance already then just don't take it for a few weeks and see what effects you have then. If still no effects then up the dosage to 900mg maximum amount. If not, then just rid it from the stack completely.
Great! I'll think I'll add this to my list of things to try. Phenibut as a lot of us know is a tricky substance when not properly dealt with. I also just recently posted a stack on here as well that was suggested by someone else, which also included ingesting Phenibut daily. I've found though that I wasn't able to handle the side effects of a low dosage for even just a few days, so now I'm gonna start over soon when I buy the free amino acid version of it. What do you suggest cycling Phenibut with once tolerance is seen?
How well has coluracetam worked for you?
Coluracetam is very good. When I take it, it improves my vision and it's kinda like "HD vision" as such, color is greatly improved along with a good mood increase. It pretty goes well with any stack! Good for depression
The stack is from this link: http://www.drugs-for...ad.php?t=188461
Stack can be modified:
Picamilon: 50-100 mg (100+ dosage slightly stimulating)
L-theanine: at least 300mg/day
Phenibut: 200-220 mg twice per day
150-200 mg of a filler such as Glycine or DMAE
Lysine: 1 g @noc.

In my personal experience:
Positives:
- Can be dissolved in Vitamin Water (a full 20oz - XXX or DragonFruit flavor preferably... fruit punch is nasty) for easy consumption throughout the day (Tastes decent and leaves a mild chemical aftertaste that goes away quickly)
- Faster absorption due to liquid solution (Don't quote me on this - I'm not 100% sure)
- Mild to moderate euphoria (setting dependent)
- Great focus
- Promotes NGF and BDNF
- Increased short term/long term memory + music appreciation
- Improved color contrast/image sharpness in the center of vision**
Negatives:
- Excessive muscle stimulation (twitching)
- Tolerance. Ingredients labelled (Optional) should not be used daily to avoid tolerance. As always, cycle.
- Possible emotional blunting. Setting dependent.
TIP: If your study session is late at night and you experience tired/dry eyes or start feeling sleepy, before taking a swig of this, try going to the bathroom and washing your face. If that's impossible, try artificial tears/lubricating eye drops (not the ones meant to reduce redness). Refresh Plus or Systane Ultra (preservative free single-use vials) works well for me.
Edit 8/9/14:
Extended description/breakdown of ingredients:
Melatonin 0.5-3mg - I included this so that it would be easier to get to sleep after consuming the stack. It is also a powerful antioxidant. If you wake up in the morning after a full night's sleep (7 hours or so) feeling sleepy or your eyes won't open, turn on your cell phone/computer and use it for a minute. the bright white light will destroy the remaining enzymes keeping you asleep. - I forgot the name behind this mechanism but it's similar to how sunlight wakes you up in the morning.
Acetyl-L-Carnitine - I included this because of its antioxidant/neuroprotective properties, as well as how it assists in the synthesis of choline. Overall synergistic with the other ingredients.
CDP-Choline/Citicoline - This is the main choline source as well as a nootropic in its own right. Increases dopamine levels, improves vision, regulates glutathione, among others.
Reduced Glutathione - Good general purpose antioxidant. I use Jarrows brand capsules for convenience.
Oxiracetam - I picked this over other racetams because of several reasons. First, it is neutral-sweet tasting and won't change the taste of the vitamin water much. Second, it is water soluble. Third, it is stronger than piracetam and requires a lower dose to achieve the same effects. Fourth, it has stimulant properties.
Noopept - This didn't do much on it's own for me. When I added it to the stack, it noticeably improved focus. Also stimulates BDNF and NGF.
Phenylpiracetam - I labelled this as optional because of the tolerance issues (builds fast). It is a more potent form of piracetam and has stimulant properties. When added to the stack, motivation to complete tasks improved immensely. Mild euphoria was also present.
Sunifiram - This is optional also because of tolerance. it provided significant focus on its own. I felt that it improved focus and increased euphoria when combined with the main stack.
Caffeine - I added this to the stack once on a whim. I have a natural caffeine tolerance so I usually require upwards of 300mg to feel threshold effects. I didn't think it would do much when I combined it but it synergized well and provided physical stimulation and mental alertness. Please dose accordingly, 200mg is strong for some individuals.
**as a result, my reading speed increased (I was reading words individually - similar to spreeder/spritz) but peripherals remained unchanged
--------------------
I hope this stack helps other college students out there. Good luck with studies!
Please post if you have tried this stack and your experiences, as well as any improvements that I can make on it. Thanks!
Advanced Glycation End-products (AGE's) occur inside the body via several pathways and/or environmental conditions of the blood. The factors in this stack have been documented to aid in the reduction of the formation of AGE's.
- A major constituent of atherosclerotic plaque is a build-up of glycated proteins (along with calcification). Taking measures to prevent glycation will give High Density Lipoproteins an upper hand in working to reverse this plaque, thereby lowering risk of stroke and ischemia.
- Diabetics have high postprandial plasma glucose levels which results in accelerated glycation of anything and everything: from hemoglobin, to organs, to random proteins, etc. As a result, secondary complications such as diabetic neuropathy, diabetic nephropathy, and diabetic retinopathy, arise. Taking measures to prevent glycation will ensure a better prognosis for the diabetic in terms of risk of developing a secondary complication.

I used to take a multi, lithium, D3, and fish oil in addition to melatonin, but because of financial considerations, and less than spectacular research results for most supps wrt to life extnesion, I had to cut back. Now I take melatonin when I go to sleep at night.



Community Forum Software by IP.Board
Licensed to: ImmInst.org




























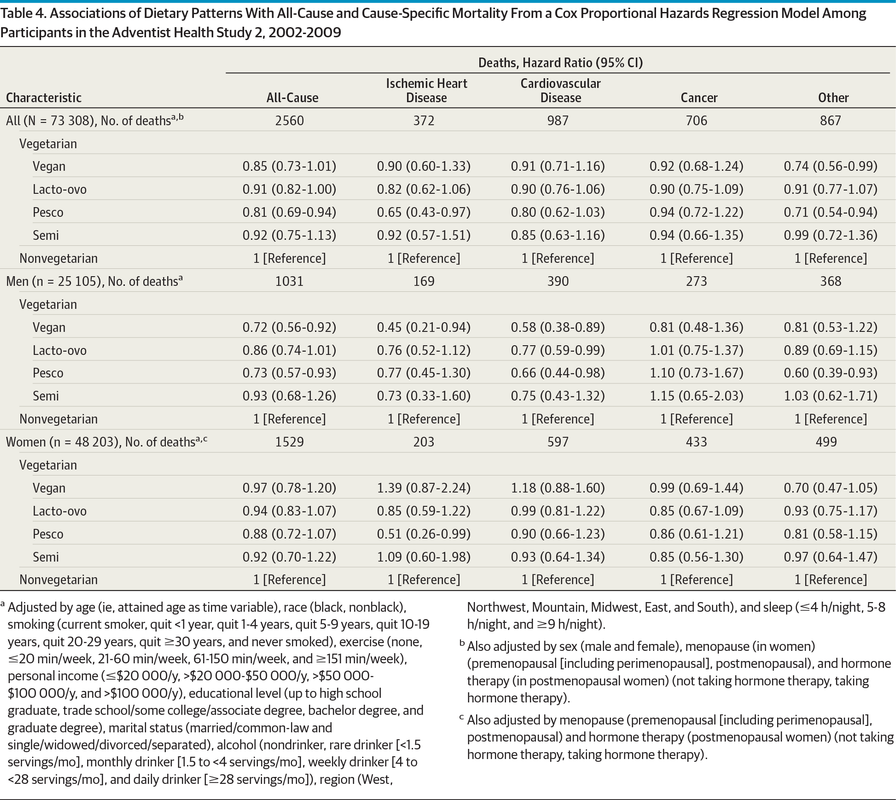{kind=link}
{kind=link}
Codex Executor, a remarkable tool, seamlessly integrates advanced AI into coding, enhancing productivity and creativity for developers.