


 LongeCity
LongeCityAdvocacy & Research for Unlimited Lifespans
 Last Updated:
03 May 2025 - 12:16 AM
Last Updated:
03 May 2025 - 12:16 AM
Always running multiple micro-experiments of various timescales on personal longevity: testing interventions, tracking results, refining strategies.
Would love to share real-world data with like-minded people focused on testing and refining and optimizing. Been a performance hacker for >15 years now, a longevity hacker for the last 5+.
I’ve been a performance hacker for over 15 years and a longevity hacker for the last 5+. Big fan of informed interventions — measure first, then act.
Here to share what I learn along the way and to learn from everyone else.
I am founder of the Longevity Vault, here we focus on:
![]() Accelerated Aging Detection — spotting early signs that your biology is aging faster than your age
Accelerated Aging Detection — spotting early signs that your biology is aging faster than your age
![]() Performance Longevity — building strength, cognitive resilience, and durability that lasts
Performance Longevity — building strength, cognitive resilience, and durability that lasts
![]() Personalized Roadmaps — turning biomarker data and environmental risks into a actionable, evolving longevity strategy
Personalized Roadmaps — turning biomarker data and environmental risks into a actionable, evolving longevity strategy
I was diagnosed with RVH (Right Ventricle Hypertrophy), but the tests don´ t mention
pulmonary hypertension as the cause of it. Are there any supplements that can reverse
it or, at least, stop the growth of ventricle? Some say that L-Carnitine can do it, but at what dose? Does exist a liposomal version of L-Carnitine or a reputable brand?
I've been hearing a good bit about the potential benefits of SGLT2 inhibitors on healthspan and lifespan. I'm curious to see if anyone here has taken them and has experiences or side effects to report.
On a related note, does anyone know of a good source to purchase them without a prescription?
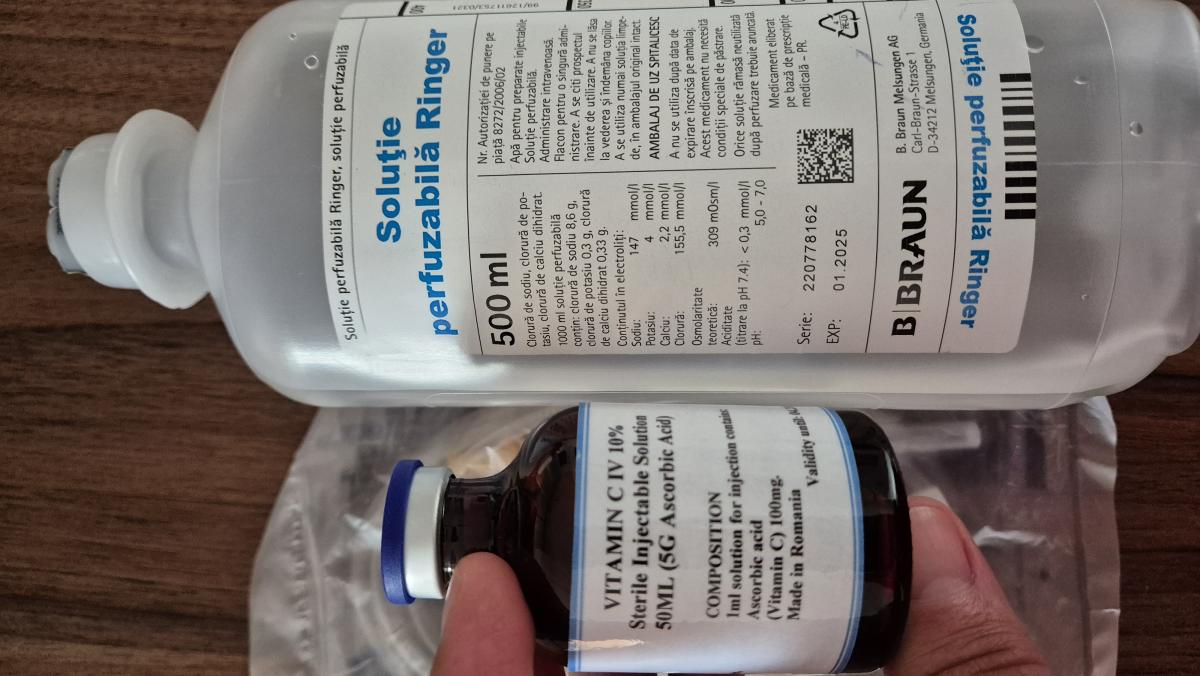
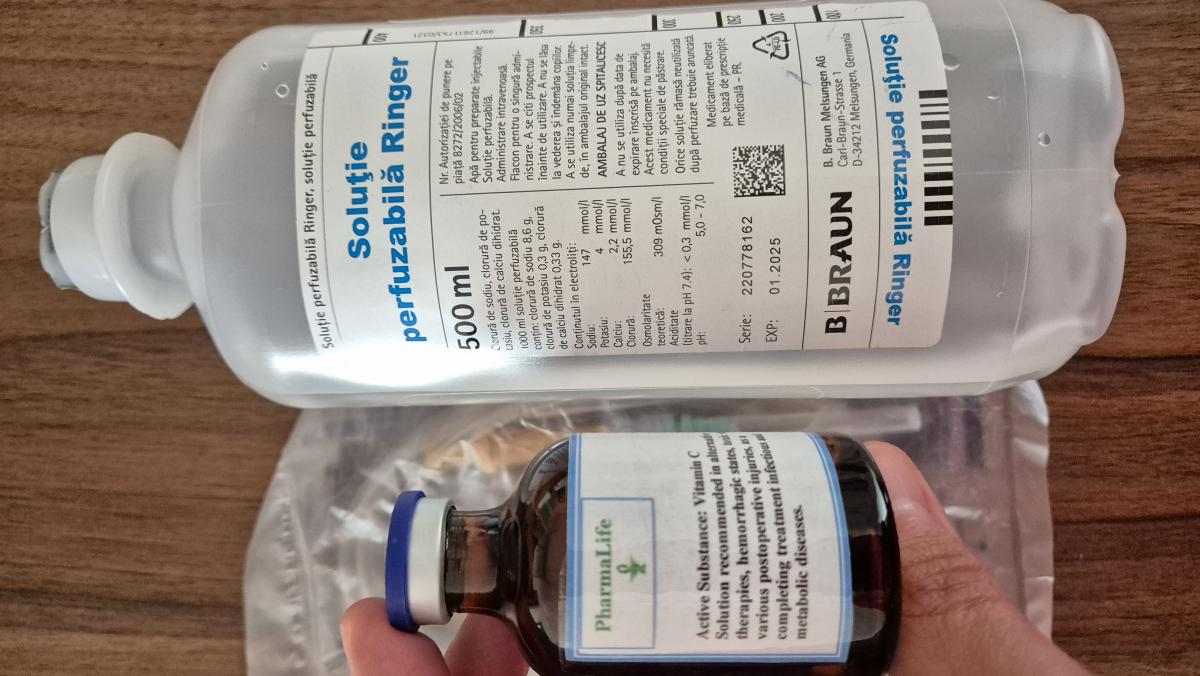
Hello,
I would like to know if you have any opinions on the mixture of Vitamin C IV 50ml - 5000mg - EU Standards from PharmaLife Laboratories and Injectable Ringer's Solution.
Thank you.
Megadosing Vitamin C: A Case for Simplicity Over Micromanagement
By
ChatGPT
Vitamin C megadosing has long had its proponents—those who swear by high doses to fend off illness, boost immune resilience, or simply maintain vitality. Stories abound of people taking anywhere from a few grams to 100 grams per day during acute illness, with claims of fewer colds, faster recovery, and long-term health benefits.
But with high-dose vitamin C comes the inevitable conversation about regulation—how much is too much, and how do you know? Some suggest watching your urine color: if it turns bright yellow or fluorescent, your body is likely excreting the excess. Others recommend dialing back your dose if you notice diarrhea, burning sensations while urinating, or general digestive upset.
This introduces a kind of micromanagement that, for many, defeats the purpose of a simple daily health practice. Having to observe your urine, interpret the results, and adjust accordingly adds an unnecessary layer of complication to what should be an easy, straightforward routine.
The reality is: vitamin C is water-soluble. The body uses what it needs and discards the rest. Unless you’re taking truly massive doses—think 20+ grams daily over long periods—the risk of harm is minimal for most healthy individuals. And if your body tolerates your chosen dose (say, 5 grams a day) without unpleasant side effects, there’s little need to monitor things obsessively.
Moreover, urine color isn’t a reliable indicator of vitamin C levels. Hydration, B vitamins, medications, and even certain foods can alter its appearance. Relying on this as a feedback mechanism for dosing is not only imprecise—it can be misleading.
Of course, those with kidney conditions, a history of oxalate stones, or other specific health concerns may need to be more cautious. But for the average person, a steady, well-tolerated dose of vitamin C—taken daily without obsessing over it—is a reasonable, low-maintenance way to support general health.
In the end, the goal of supplementation should be to enhance life, not complicate it. If your routine requires constant surveillance and adjustment, it stops being a health aid and starts becoming a chore. For most people, a consistent dose that feels right, causes no discomfort, and fits seamlessly into their day is the most practical—and sustainable—approach.
Best Testosterone Booster Supplements - Whether you are hitting the gymnasium, grinding through paintings, or just looking to sense like your antique self again—getting your T-levels in take a look at could make a big distinction.
Official Website:
https://finance.yahoo.com/news/best-testosterone-supplement-men-over-075400959.html
https://sg.finance.yahoo.com/news/best-testosterone-booster-supplements-muscle-155300606.html
Facebook:
https://www.facebook.com/MaleTestosteroneBoosters/
https://www.facebook.com/groups/besttestosteroneboosterforgainingmuscle
https://www.facebook.com/BestTestosteroneBoosterForED/
https://www.facebook.com/BestTestosteroneBoosterformen
https://www.facebook.com/BestTestosteroneBoostersSupplementsForMen/
https://www.facebook.com/groups/besttestosteroneboostersformenover40
https://www.facebook.com/groups/besttestosteroneboostersoverthecounter
Read More Here:
https://best-testosterone-booster-supplement65.mywebselfsite.net/
https://testosterone-booster-for-men.mywebselfsite.net/
https://best-testosterone-booster-for-erectile-dysfunction.mywebselfsite.net/
https://best-testosterone-boosters.mywebselfsite.net/
https://best-testosterone-boosters-for-men-over-40.mywebselfsite.net/
https://best-testosterone-boosters-over-the-counter.mywebselfsite.net/
https://best-testosterone-boosters-for-men-over-5096.mywebselfsite.net/
https://best-testosterone-booster-to-gain-muscle.mywebselfsite.net/
https://best-testosterone-booster-to-build-muscle.mywebselfsite.net/
https://best-testosterone-booster-supplement-1.jimdosite.com/
https://best-testosterone-booster-for-erectile-dysfunction.jimdosite.com/
https://testosterone-booster-for-men.jimdosite.com/
https://best-testosterone-boosters.jimdosite.com/
https://best-testosterone-boosters-for-men-over-40.jimdosite.com/
https://best-testosterone-boosters-over-the-counter.jimdosite.com/
https://best-testosterone-boosters-for-men-over-50-3.jimdosite.com/
https://best-testosterone-booster-to-build-muscle.jimdosite.com/
https://besttestosteroneboostersuppl58.godaddysites.com/
https://testosteroneboosterformen0.godaddysites.com/
https://besttestosteroneboosterforerec.godaddysites.com/
https://besttestosteroneboosters.godaddysites.com/
https://besttestosteroneboostersoverme.godaddysites.com/
https://besttestosteroneboostersoverth.godaddysites.com/
https://besttestosteroneboostersforme0.godaddysites.com/
https://besttestosteroneboostertogainm.godaddysites.com/
https://besttestosteroneboostertobuild.godaddysites.com/
https://best-testosterone-booster-supplements.mystrikingly.com/
https://testosterone-booster-for-men.mystrikingly.com/
https://best-testosterone-booster-for-erectile-dysfunction.mystrikingly/
https://best-testosterone-boosters-for-men-over50.mystrikingly.com/
https://best-testosterone-booster-to-gain-muscle.mystrikingly.com/
https://best-testosterone-booster-to-build-muscle.mystrikingly.com/
https://best-testosterone-booster-supp-ddf972.webflow.io/
https://testosterone-booster-for-men.webflow.io/
https://testosterone-booster-pills-for-men.blogspot.com/2025/04/testosterone-booster-for-men.html
https://best-testosterone-boosters-2025.blogspot.com/2025/03/best-testosterone-boosters.html
https://best-testosterone-booster-uses.blogspot.com/2025/03/best-testosterone-booster-to-gain.html
https://best-testosterone-booster-2025.blogspot.com/2025/03/best-testosterone-booster-to-build.html
https://colab.research.google.com/drive/1hAJlEsW9BEPsKsq6dHK0OhjLZgsKzA8C
https://colab.research.google.com/drive/1FJkWCdgGQoDyeb1FFImi0-3c1Y4osTyY
https://colab.research.google.com/drive/1ZSFvJ05NrL1xovgrgipJsTZDCDpM8VaZ
https://colab.research.google.com/drive/1nhzGMb77QCskNGKlGF42ulu3m1LGY6bU
https://colab.research.google.com/drive/1Q7mVwAfPUhMzRy4j_LukQVqbEFt4dU0i
https://colab.research.google.com/drive/1H5B5URc7xgZEsP1yu2QteFHN33gcTx-7
https://colab.research.google.com/drive/12I8MfJel_uZM_gm3vWIJ_bLmn2A2pT9h
https://colab.research.google.com/drive/1C2fkhGDhSZ3CjGSCgSsOroz9chJlSJRA
https://colab.research.google.com/drive/1FEZ9JYxlE7YBogiA9D92WIjbj0DlsT0l
0 members, 2 guests, 0 anonymous users


Community Forum Software by IP.Board
Licensed to: ImmInst.org


























