To offer more food for thought, another comment to bio-availability:
there are 2 studies done for bio-availability of Glucosamine (GS) in humans; the more important one being:
"Glucosamine oral bioavailability and plasma pharmacokinetics after increasing doses of crystalline glucosamine sulfate in man": https://www.oarsijou...0193-7/fulltext
Their main findings:
- GS got an elimination half-life of about 15 hours in humans
- an oral doses up to 1,5 gram in on sitting is readily absorbed and increases plasma concentration of GS proportionally compared to 0,75 gram
- oral intake of 3 gram of GS in one sitting did result in a less than proportional increase in plasma levels
This indicates, that you might want to spread out taking a GS intake of 3 gram or more per day - i.e. a little in the morning and a little in the evening - to get the most out of it.
To make you scratch your head a little more, let's have a look at the actual GS-uptake mechanism. This picture illustrates the structure of glucosamine to the left and glucose to the right. Both are simple molecules - the only difference being the exchange of on hydroxy-group by one amino-group:

Glucosamine in principle utilities the same cellular transporters as glucose. But there is one strange difference: GLUT2 - a glucose transporter that is especially prevalent in the nutrient absorbing small intestines and does not require insulin to be activated - is highly sensitive to glucosamine:
"GLUT2 is a high affinity glucosamine transporter"
https://www.scienced...014579302030582
According to above study this glucose transporter actually is 21-fold as sensitive to glucosamine as it is for glucose itself - meaning glucose requires a 21-fold concentration in the medium to be transported at the same rate as is glucosamine. The liver got an elevated concentration for GLUT2 as well. This combination could be the explanation for the good bio-availability of oral glucosamine in blood plasma.
As mentioned before, in one mice study, administering the human equivalent of 3 gram glucosamine per day resulted in more active autophagy than caloric restriction. The results looked like this:
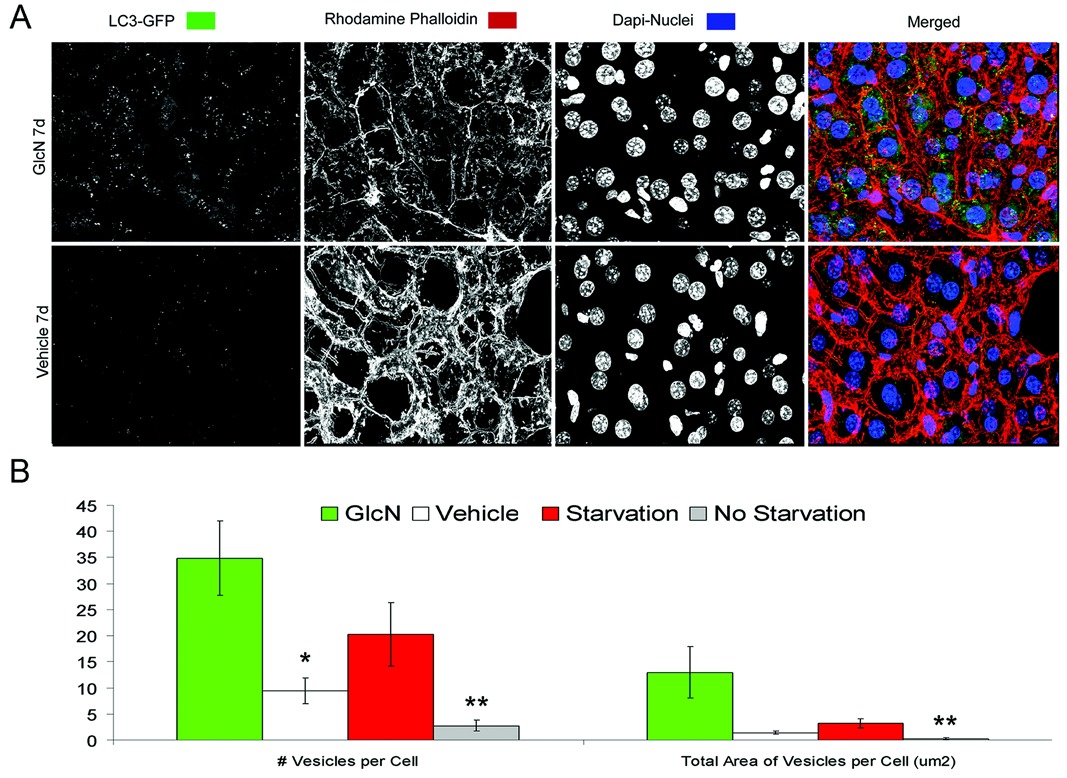
yellow - glucosamine
white - controls
red - caloric restriction
grey - a different mouse strain as further controls
Although GS and glucose are structurally almost identical, the effects are very markedly different. The controls got glucose as part of their lab diet (as did the treatment groups). Starving the mice on a water-only fast (and consequently no glucose) did increase AP. But using a rather small dose of GS in addition to a normal glucose intake resulted in a considerably stronger AP.
It appears, that GS got an effect on AP that goes beyond competing against glucose. So it could be more to GS than just mimicking a reduced carb diet.
Glucosamine:
- much safer than metformin
- better life extension effects in mice than metformin
- life-extension in a prospective cohort study in healthy humans - 22% reduced all-cause mortality rate in on analysis of the VITAL-data (or even up to 49% reduced all-cause mortality rate if you believe the analysis of only the participants that did no use NSAID... but I personally think that's just a statistical fluke)
- and the cancer-studies concluded, that there is a dose-depended effect - the more you take, the better the benefits... and GS is very safe
- potentially better AP than caloric restriction using a rather small dose...
Give me a reason, why anyone is taking metformin for purely life-extension purposes - but not glucosamine. Or Vitamin K2 (it's got less evidence than GS going for it). Or a dozend other less impressive supplements, that even deliver less impressive safety-records.
Edited by Guest, 22 May 2019 - 09:07 PM.































































