































.
F U L L T E X T S O U R C E : AgING
Abstract
From the dawn of civilization, humanity has dreamed of immortality. So why didn’t the discovery of the anti-aging properties of mTOR inhibitors change the world forever? I will discuss several reasons, including fear of the actual and fictional side effects of rapamycin, everolimus and other clinically-approved drugs, arguing that no real side effects preclude their use as anti-aging drugs today. Furthermore, the alternative to the reversible (and avoidable) side effects of rapamycin/everolimus are the irreversible (and inevitable) effects of aging: cancer, stroke, infarction, blindness and premature death. I will also discuss why it is more dangerous not to use anti-aging drugs than to use them and how rapamycin-based drug combinations have already been implemented for potential life extension in humans. If you read this article from the very beginning to its end, you may realize that the time is now.
“If you wait until you are ready, it is almost certainly too late.” Seth Godin
In one short-lived mutant strain of mice, the mTOR inhibitor rapamycin (known in the clinic as Sirolimus) extends maximum life span nearly three-fold [1]. Albeit less spectacularly, rapamycin also prolongs life in normal mice as well as in yeast, worms and flies, and it prevents age-related conditions in rodents, dogs, nonhuman primates and humans. Rapamycin and its analog, everolimus, are FDA approved for human use and have been used safely for decades. In 2006, it was suggested that rapamycin could be used immediately to slow down aging and all age-related diseases in humans [2], becoming an “anti-aging drug today” [3].
But rapamycin was unlucky
Rapamycin known in the clinic as Rapamune or Sirolimus, was unlucky from the start, however. Twenty years ago, it was labeled an immunosuppressant and used to treat renal transplant patients. If rapamycin had been labeled an immunomodulator and anti-inflammatory drug instead, it would sound much more appealing now. At anti-aging doses, rapamycin “eliminates hyperimmunity rather than suppresses immunity” or, more figuratively, it “rejuvenates immunity” [2]. This enables rapamycin and everolimus, a rapamycin analog, to act as immunostimulators [4–6], improving immunity in cancer patients [7] and the elderly [8,9]. For example, rapamycin reduces the risk of CMV infection in organ transplant patients [10–12], improves antipathogen and anticancer immunity in mice [13–15], prolongs lifespan in infection-prone mice [16] and protects aged mice against pneumonia [17]. Rapamycin also inhibits viral replication [18,19]. As a noteworthy example, rapamycin inhibits replication of the 1918 flu virus (the deadliest flu virus in history) by 100-fold [19], and also protects against lethal infection with influenza virus when administered during vaccination [13]. Still, as Dr. Allan Green advises, patients taking rapamycin should be carefully monitored for skin and subcutaneous bacterial infections, which should be treated with antibiotics https://rapamycintherapy.com.
Twenty years ago, it was thought that rapamycin might increase the risk of cancer (see a forthcoming review “Understanding the side effects of rapamycin”). Despite that concern, it was revealed that rapamycin actually prevents lymphoma and some types of cancer in transplant patients [20–27]. Currently, in fact, rapamycin analogs, everolimus and temsirolimus, are widely used in cancer therapy. Furthermore, rapamycin is the most effective known cancer-preventive agent in mice [25,28–32] extending the lifespan of cancer-prone mice [33–36]. It has even been suggested that rapamycin extends lifespan by preventing cancer [37].
Nevertheless, social media often warn that although rapamycin prevents cancer, its use to prevent cancer may come at the cost of getting cancer. This self-contradiction miscites a twenty-year-old warning by the FDA for all drugs marketed as immunosuppressants (including rapamycin and everolimus): “Increased susceptibility to infection and the possible development of malignancies such as lymphoma and skin cancer may result from immunosuppression.” This statement does not say that rapamycin or everolimus cause malignancies. (Just read it again). Although rapamycin and its analogs are now approved by the FDA for treatment of cancer and lymphomas, the rumors that these drugs may cause cancer persist. To my knowledge, no study has shown that mTOR inhibitors cause cancer.
At this point, most scientists agree that rapamycin is not counterindicated because of concerns about immunosuppressive effects. But a new objection against rapamycin has emerged, namely that rapamycin may cause diabetes. As discussed in detail [38], the new wave of “fear of rapamycin” is groundless. So, what are the metabolic effects of rapamycin?
Metabolic effects or rapamycin and starvation
When it is over-activated by nutrients and insulin, mTOR acts via S6K to inhibit insulin signaling, thereby causing insulin resistance [39–44]. Acute treatment with rapamycin abrogates insulin resistance in cells and animals including humans [45–51]. One study showed that chronic treatment with rapamycin may also prevent insulin resistance [52]. However, in some (but not all) rodent models, chronic treatment with rapamycin can also cause glucose intolerance and even insulin resistance [53–56]. This was interpreted as a deleterious side effect or even type 2 diabetes (T2D). Actually, however, these metabolic changes are features of benevolent starvation pseudo-diabetes (SPD), which was described 170 years ago in fasted animals and later in humans [57,58]. During prolonged fasting, utilization of glucose by non-brain tissues must be suppressed to ensure an adequate supply to the brain. When a fasted animal or human is then given a meal, glucose appears in the urine (glycosuria), which is a canonical symptom of diabetes. But this is because prolonged fasting (starvation) leads to decreased insulin secretion and to insulin resistance, and subsequent re-feeding then causes transient hyperglycemia and glycosuria. This SPD can be caused not only by prolonged fasting, but also by severe restriction of calorie and carbohydrate intake [38]. For example, severe calorie restriction can cause diabetes-like glucose intolerance [59]. Despite that, very low calorie diets are the most effective treatments for type 2 diabetes [60–62]. Some researchers re-discovered SPD in obese patients on strenuous weight loss program and erroneously warned that low calorie diets cause type 2 diabetes [63].
The obligatory symptom of starvation is ketosis, as ketones substitute for glucose as the main fuel for the brain. The ketogenic diet, a promising treatment for diabetes and obesity in humans, can cause symptoms of SPD in rodents (see for references [64]). Once again, some researchers warned that the ketogenic diet can favor type 2 diabetes [65]. As discussed, such warnings may not be justified [64,66–68].
Rapamycin can be viewed as a partial starvation-mimetic [69–71]. It is therefore predictable that, under some conditions, prolonged treatment with rapamycin may lead to the emergence of SPD [72]. This has been confirmed in rapamycin-fed mice, which developed insulin resistance, glucose intolerance and mild hyperglycemia [54]. Nevertheless, rapamycin-fed mice lived longer and thus were healthier than mice fed a standard diet [54]. It is not completely clear why SPD was observed in only some studies and was not observed in other studies (see for references [38,73]).
Importantly, SPD is reversible and does not lead to complications. Furthermore, rapamycin reduces the incidence of diabetic complications such as diabetic nephropathy in rodents [42,74–85]. In healthy elderly humans, chronic treatment with rapamycin or everolimus did not cause hyperglycemia [8,9,86]. On the contrary, the risk of hyperglycemia was lower in the mTOR inhibitor treatment group than the placebo group [9].
In some cancer patients, high doses of rapamycin or everolimus can cause hyperglycemia, which is usually mild (grade 1-2) and reversible, and does not lead to treatment interruption [87–89]. Hyperglycemia is a common side effect of many oncotargeted drugs and is not a manifestation of diabetes. Everolumus, for example, can cause hyperglycemia by decreasing insulin production [89].
To summarize, chronic treatment with high doses of rapamycin may cause symptoms of reversible SPD. Diet-induced SPD, at least, is beneficial and therapeutic. Rapamycin-induced SPD is a relatively rare side effect and probably can be avoided by administering the drug intermittently or at lower doses, and if SPD does occur, it can be reversed by discontinuation of the drug.
In some studies in transplant patients, rapamycin (sirolimus) and everolimus did not increase the risk of diabetes [90–96]. In one study, no patient, out of 21 patients treated with rapamycin, developed diabetes, while the incidence of diabetes was 7% in patients treated with either cyclosporine or tacrolimus [96]. Most importantly, cyclosporine- or tacrolimus-induced diabetes resolved in 80% of patients after conversion from tacrolimus/cyclosporine to rapamycin (sirolimus) [96].
On the other hand, a large retrospective study reported an association between Medicare billing for diabetes treatment and rapamycin use, implying that rapamycin may increase the risk of diabetes [97]. However, this association was explained by the interaction between rapamycin and calcineurin inhibitors, which increase each other’s levels [96,98,99]. Consequently, it remains unclear whether rapamycin per se increases the risk of diabetes in transplant patients [96]. Moreover, this is further complicated by the fact that most transplant patients develop type 2 diabetes spontaneously without rapamycin treatment [100].
Rapamycin is not much more dangerous than ordinary drugs
If used properly, rapamycin is not much more dangerous than ordinary aspirin. Aspirin, one of the most widely used nonprescription medications, may cause numerous side effects, including life threatening gastric bleeding. The manufacturer lists as possible side effects: ringing in ears, confusion, hallucinations, seizure, severe nausea, vomiting, bloody stools, coughing up blood, fever and swelling. Still, millions of people take aspirin daily to prevent cardiovascular disease and cancer. It was calculated that the benefits of aspirin are greater than their risks [101,102]. I believe the benefits of the anti-aging effects of rapamycin/everolimus may even be greater (Figure 1).
Potential risk vs benefits of rapamycin-based anti-aging therapy. Pros and Cons: Potential benefits of rapamycin may outweigh its risks.

Figure 1. Potential risk vs benefits of rapamycin-based anti-aging therapy. Pros and Cons: Potential benefits of rapamycin may outweigh its risks.
In the case of rapamycin and everolimus, the most worrying side effects have not been confirmed. At low doses [8,9,86], or when administered as a single high dose [103], no side effects have been detected so far in the elderly. At high doses, rapamycin and everolimus slow cell proliferation, which decreases blood cell counts. As a result, mild and reversible thrombocytopenia (low platelet count), anemia and leukopenia are their most common side effects. But a mild reduction of platelets may be beneficial. In fact, one of the intended effects of aspirin is a decrease in platelet function.
There is one crucial reason why the side effects of rapamycin are exaggerated. The frequency of rapamycin side effects has often been estimated in studies lacking a placebo group. In cancer and transplant patients, numerous effects ascribed to rapamycin, such as fatigue (asthenia), for example, are often caused by the disease itself. In a placebo study of healthy volunteers, the placebo group reported more side effects such as fatigue than did the rapamycin group [104]. In recent placebo-controlled studies in healthy elderly people, no side effects were noticed as compared to placebo [9,86].
While aspirin may cause gastric ulceration and bleeding, rapamycin may cause stomatitis and mycositis (ulceration of the mucous membranes of the mouth and the digestive tract) when used at high doses or chronically. A rare side effect of rapamycin is noninfectious interstitial pneumonitis [105]. And by inhibiting neutrophil function, rapamycin may increase the severity of bacterial infections [106]. These side effects require rapamycin’s discontinuation. For antiaging purposes, however, rapamycin may be used either intermittently (e.g., once a week) or at low daily doses and can be discontinued if any unpleasant effects occur.
From a single dose to intermittent schedules
Although nearly all drugs, including nonprescription drugs such as aspirin, can be fatal at sufficiently high doses, there are no known fatal cases of acute rapamycin (sirolimus) overdose [103]. For example, in a failed suicide attempt, an 18-year-old woman ingested 103 rapamycin tablets (103 mg), and the only detected effect was an elevation in total blood cholesterol [103]. In rats, rapamycin’s LD50, a measure of drug lethality, could not be determined because it is higher than 2500 mg/kg. While a single dose of rapamycin is safe, it is sufficient to extend life and decrease obesity in several rodent models [1,107]. Furthermore, transient treatment with rapamycin can be long lasting, extending the lifespan and preventing obesity long after drug discontinuation [107–112]. The magnitude of life extension by rapamycin depends mostly on reaching a high peak blood level [113]. A similar conclusion was reached by a study of rapamycin use in obesity [112]. It was suggested in 2008 that a pulse (intermittent) schedule of rapamycin administration would improve regeneration of stem cells [114] while avoiding mTORC2 inhibition [54,115].
Therefore, to avoid side effects and maximize anti-aging effects [110], a feasible approach would be to prolong intervals between rapamycin administrations while keeping the total dose constant. For example, instead of daily administration, a weekly administration of a higher dose can be suggested to achieve a high peak blood level, followed by drug-free period to avoid undesirable effects. Still, everyday treatment of the elderly (1 mg/day for several weeks) was not associated with side effects and has been shown to be safe [86]. Similar results were achieved with low doses of other mTOR inhibitors [9]. Another option is an alternating schedule; for example, a 3- month course of weekly rapamycin alternating with a rapamycin-free month. Finally, anti-aging schedules can be very flexible to fit an individual patient. The optimal anti-aging dose is a personalized maximum dose that does not cause side effects in a particular patient (Figure 2).
Optimal dose of rapamycin for maximal net benefits. Life extension by rapamycin is dose-dependent in rodents. The higher the dose, the higher the anti-aging benefits, including cancer prevention and life extension. In humans, side effects are dose-dependent and net benefits could potentially decrease at very high doses. This point of the highest net benefit is the optimal dose. The optimal dose varies in different individuals due to the variability of potential side effects. Thus, the optimal dose in a particular individual is determined by the emergence of side effects. The treatment can be viewed as life-long phase I/II clinical trial.
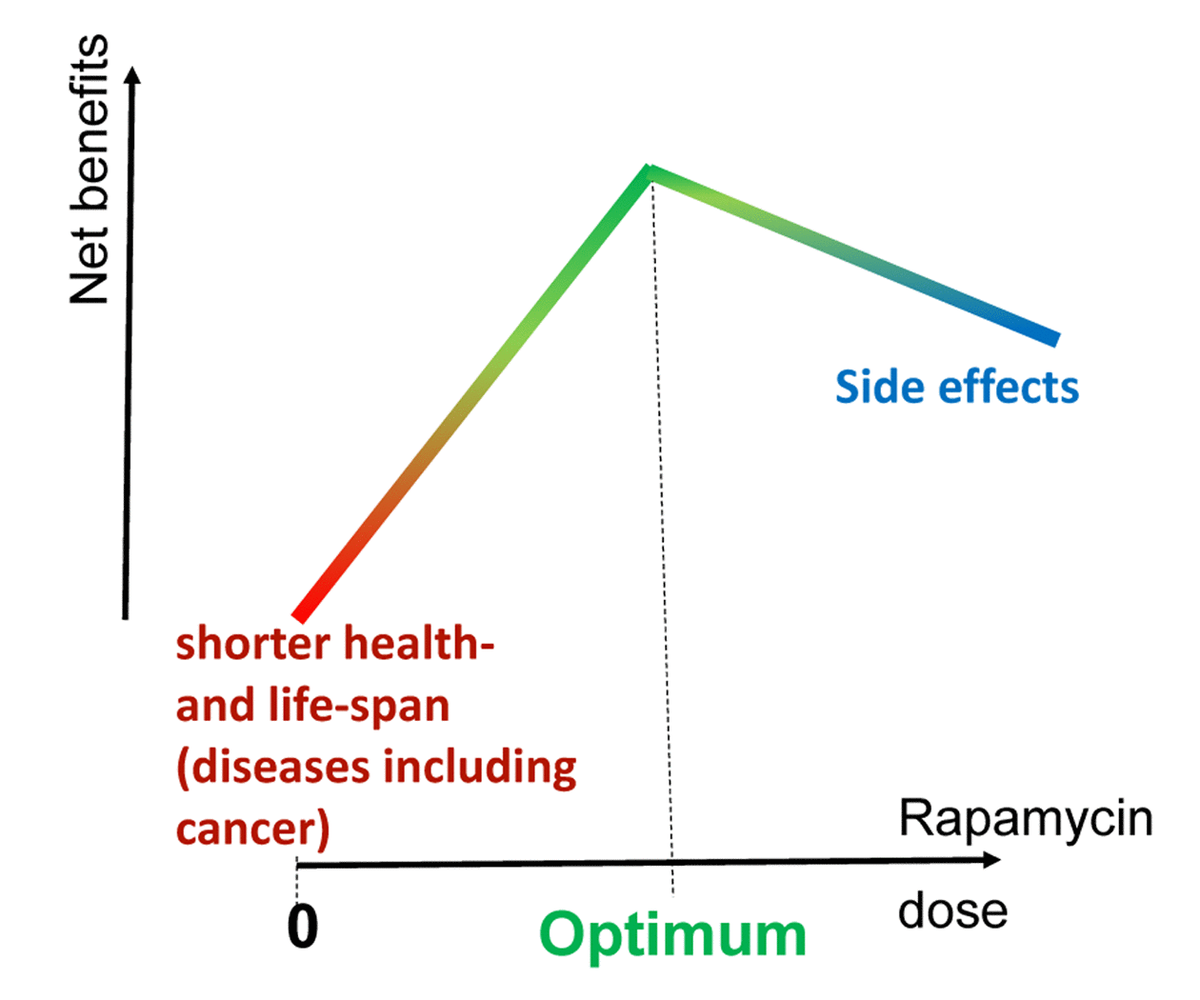
Figure 2. Optimal dose of rapamycin for maximal net benefits. Life extension by rapamycin is dose-dependent in rodents. The higher the dose, the higher the anti-aging benefits, including cancer prevention and life extension. In humans, side effects are dose-dependent and net benefits could potentially decrease at very high doses. This point of the highest net benefit is the optimal dose. The optimal dose varies in different individuals due to the variability of potential side effects. Thus, the optimal dose in a particular individual is determined by the emergence of side effects. The treatment can be viewed as life-long phase I/II clinical trial.
In conclusion, the side effects of rapamycin are well-known and reversible. When used on an anti-aging schedule, side effects may be absent but, if not, they may be mitigated by combining rapamycin with other anti-aging drugs (metformin, statins) or by temporarily discontinuing it.
Noteworthy, the alternative to the reversible (and avoidable) side effects of rapamycin/everolimus are the irreversible (and inevitable) effects of aging. And by living longer, our generation will benefit from future anti-aging discoveries (Figure 1).
But the fear of nonexistent side effects is not the only reason the use of mTOR inhibitors for life extension has been questioned. The second reason is that there is rightful skepticism about any claims made about anti-aging drugs because thousands of anti-aging remedies have already failed. What then makes rapamycin different?
.../...
F O R T H E R E S T O F T H E A R T I C L E , P L E A S E V I S I T T H E S O U R C E .
.


















