































.
F U L L T I T L E :
Compounds that extend longevity are protective in neurodegenerative diseases and provide a novel treatment strategy for these devastating disorders
O P E N A C C E S S S O U R C E : Mechanisms of Ageing and Development
Highlights
• Aging is the greatest risk factor for the development of neurodegenerative disease.
• Multiple compounds have been shown to extend lifespan in model organisms.
• These lifespan-extending compounds have been shown to be neuroprotective in animal models of disease.
• Targeting the aging process may be an effective strategy to treat neurodegeneration.
Abstract
While aging is the greatest risk factor for the development of neurodegenerative disease, the role of aging in these diseases is poorly understood. In the inherited forms of these diseases, the disease-causing mutation is present from birth but symptoms appear decades later. This indicates that these mutations are well tolerated in younger individuals but not in older adults. Based on this observation, we hypothesized that changes taking place during normal aging make the cells in the brain (and elsewhere) susceptible to the disease-causing mutations. If so, then delaying some of these age-related changes may be beneficial in the treatment of neurodegenerative disease. In this review, we examine the effects of five compounds that have been shown to extend longevity (metformin, rapamycin, resveratrol, N-acetyl-L-cysteine, curcumin) in four of the most common neurodegenerative diseases (Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, amyotrophic lateral sclerosis). While not all investigations observe a beneficial effect of these compounds, there are multiple studies that show a protective effect of each of these lifespan-extending compounds in animal models of neurodegenerative disease. Combined with genetic studies, this suggests the possibility that targeting the aging process may be an effective strategy to treat neurodegenerative disease.

Abbreviations
4E-BP4E = binding protein
6OHDA6 = hydroxydopamine
AD = Alzheimer’s disease
Aβ = Amyloid beta
ALS = amyotrophic lateral sclerosis
AMP = AMP-activated protein kinase
APP = amyloid precursor protein
ApoE3 = apolipoprotein E3
ApoE4 = apolipoprotein E4
ATG13 = autophagy Related 13
DLB = dementia with Lewy bodies
eIF4E = eukaryotic Translation Initiation Factor 4E
FKBP12 = 12 kDa FK506-binding protein
FUS = fused in sarcoma
GSH = glutathione
HD = Huntington’s disease
HO-1 = heme oxygenase-1
Htt = huntingtin
JNK = c-Jun N-terminal kinase
LRRK2 = leucine-Rich Repeat Kinase
MDA = malondialdehyde
MPP+1 = methyl-4-phenylpyridinium MPTP1-methyl-4-phenyl-1,2,3,6 tetrahydropyridine
mTOR = mammalian target of rapamycin
NAC = N-acetyl-L-cysteine
PCG-1α = peroxisome proliferator-activated receptor gamma coactivator 1-alpha
PD = Parkinson’s disease
ROS = reactive oxygen species
S6K = ribosomal protein S6 kinase
SIRT1 = sirtuin-1
SN = substantia nigra
SNCA = synuclein alpha
SOD1 = Superoxide dismutase 1
T2DM = Type 2 Diabetes Mellitus
TDP-43 = TAR DNA-binding protein 43
TOR = target of rapamycin
TORC1 = Target of rapamycin complex 1
TORC2 = Target of rapamycin complex 2
ULK1 = Unc-51 Like Autophagy Activating Kinase 1
1. Introduction
Neurodegenerative diseases are characterized by the progressive dysfunction and degeneration of neurons in the brain and peripheral nervous system. These devastating disorders affect more than 50 million people worldwide. Although genetic and environmental risk factors have been identified for all of these diseases, the pathogenesis of these diseases remains incompletely understood. While symptomatic treatments are available for some of these disorders, there are currently no disease-modifying treatments that can slow disease progression or halt the loss of neurons. As aging is the greatest risk factor for many of these adult-onset neurodegenerative diseases, including Alzheimer’s and Parkinson’s disease, it will be important to determine if interventions that extend lifespan can protect against these devastating disorders.
1.1. Alzheimer’s disease (AD)
AD is the most common neurodegenerative disorder. AD and other dementias affect 40 to 50 million people worldwide (Nichols et al., 2019). While there are rare cases of early-onset familial AD affecting individuals under 65 years of age, AD typically affects individuals over 65 years of age, and over 95% of AD cases are sporadic cases. Moreover, the risk of AD doubles every 5 years after the age of 65. AD is characterized by difficulties with memory, language, problem-solving and cognitive functions. Brains of AD patients are marked by amyloid plaques, which contain amyloid beta (Aβ), and neurofibrillary tangles, which contain hyperphosphorylated tau. Degeneration starts in the medial temporal lobe, spreads to the hippocampus and amygdala, and eventually to other parts of the brain (Lehéricy et al., 1994; Scahill et al., 2002). Decades of research point towards Aβ aggregation as an important contributor to AD pathogenesis. This could be due to either increased production of Aβ or decreased clearance of Aβ. Aβ oligomers are toxic in neuronal culture (Lambert et al., 1998), contribute to memory deficits in mice (Lesne et al., 2006), and correlate with neurodegeneration in AD patients (McLean et al., 1999). However, therapies targeting Aβ have so far failed in clinical trials shifting the field towards studying other contributing factors to AD pathogenesis, such microbial infection (Fulop et al., 2018), dysfunctional vasculature (Zlokovic, 2011), and environmental pollution (Peters et al., 2019). Currently, AD treatments can treat the symptoms but fail to slow disease progression or cognitive decline.
1.2. Parkinson’s disease (PD)
PD is the second most common neurodegenerative disease, affecting as many as 10 million individuals worldwide. PD is a movement disorder, which is characterized by the degeneration of dopaminergic neurons within the substantia nigra (SN) and the formation of aggregates, called Lewy bodies, which are primarily composed of a protein called α-synuclein. While interventions are available to control the motor symptoms of PD, there are currently no treatments that can prevent the loss of dopamine neurons or halt the progression of this disease. A growing number of genes have been shown to contribute to the development of PD including SNCA, the gene that encodes α-synuclein (Polymeropoulos et al., 1997; Singleton et al., 2003), and LRRK2, which encodes a Leucine-Rich Repeat Kinase (Paisan-Ruiz et al., 2004; Zimprich et al., 2004). Nonetheless, the majority of PD cases are considered to be sporadic, as only ∼10% of patients have a direct genetic cause. Although the pathogenesis of PD is incompletely understood, aging is the greatest risk factor for the development of PD (Collier et al., 2011; Driver et al., 2009). Individuals typically do not develop PD until they are 50 years and older. The prevalence of PD is 0.3% in the general population but increases to 1% for those over 60 years, and 4% for those more than 80 years of age. A role for aging in PD is also suggested by the fact that there are many commonalities between PD and normal aging (Rodriguez et al., 2015) including protein aggregation (Tan et al., 2009), increased oxidative stress (Zhou et al., 2008), decreased mitochondrial function (Henchcliffe and Beal, 2008), dysfunction of the proteasome (Cook and Petrucelli, 2009), and impairment of autophagy (Pan et al., 2008).
1.3. Huntington’s disease (HD)
HD is the most common inherited neurodegenerative disorder, affecting approximately one in 10,000 individuals. Unlike more widespread disorders, such as AD and PD, HD is entirely due to a single genetic cause: a trinucleotide CAG repeat expansion in the huntingtin (HTT) gene. HD is an autosomal dominant disorder which causes motor dysfunction, cognitive deficits, and neuropsychiatric abnormalities. In the brain, HD is characterized by selective degeneration of the striatum and the cortex as well as the appearance of mutant Htt aggregates. Following the discovery of the HTT gene, a number of genetic animal models of HD have been generated to study disease mechanisms and treatment (Brignull et al., 2006; Faber et al., 1999; Fernandez-Funez et al., 2000; Gray et al., 2008; Mangiarini et al., 1996; Marsh et al., 2000; Parker et al., 2001; Satyal et al., 2000; Schilling et al., 1999; Slow et al., 2003). Nonetheless, the pathogenesis of HD is not completely understood, and there are currently no approved disease-modifying therapies. An important unanswered question is why HD takes decades to develop when the disease-causing mutation is present in all cells throughout life. The average age of onset for HD is 40 years of age, progressing inevitably to death 10-15 years thereafter. A role for aging in the pathogenesis of HD is supported by the fact that multiple functions that decline with age have also been implicated in the disease including decreased proteasome activity, decreased autophagy, decreased chaperone function, mitochondrial dysfunction, increased oxidative stress, and increased protein aggregation (Bence et al., 2001; Browne and Beal, 2006; DiFiglia et al., 1997; Kitamura et al., 2006; Panov et al., 2002; Ravikumar et al., 2004).
1.4. Amyotrophic lateral sclerosis (ALS)
ALS is the most common adult-onset motor neuron disease, affecting one in 50,000 people in Western countries (Chiò et al., 2013). ALS is caused by degeneration of upper and lower motor neurons, leading to loss of voluntary movement. The disease progresses swiftly, with patients succumbing to the disease within an average of three years after diagnosis (del Aguila et al., 2003). Roughly 95% of ALS cases are sporadic (Byrne et al., 2011), with the largest known risk factor for sporadic ALS being aging. Both sporadic and familial ALS-onset typically occurs between 40-70 years of age (Alonso et al., 2009). The cellular pathogenesis of ALS is unclear, but a cellular hallmark of ALS is cytoplasmic aggregates in the motor neurons of patients. Over 97% of sporadic ALS cases have aggregates containing the RNA/DNA binding proteins TAR DNA-binding protein 43 (TDP-43) or fused in sarcoma (FUS) (Deng et al., 2010; Neumann et al., 2006). Mutations in FUS or the TDP-43-encoding gene, transactive response DNA binding protein (TARDBP), can cause familial ALS (Guerrero et al., 2016), and have been used to generate animal models of the disease. Animal models of ALS have also been generated using aggregation-inducing mutations in superoxidase dismutase 1 (SOD1), as this is a common genetic cause of ALS in humans. However, SOD1 animal models and patients do not exhibit FUS aggregation, making it unclear if SOD1 ALS animals are an accurate model for sporadic ALS (Deng et al., 2010). Work with these ALS models and others have identified defects in RNA regulation, phase-separation, nucleocytoplasmic trafficking, stress granule regulation, selective autophagy, and cytoskeleton dynamics (Kim and Taylor, 2017; Taylor et al., 2016; Van Damme et al., 2017). It is unclear if one of these pathways is the driving cause of ALS or if they each contribute to ALS pathogenesis.
1.5. Targeting aging pathways as a therapeutic strategy for neurodegenerative disease
While aging was traditionally considered to be a stochastic process of damage accumulation, it is now clear that lifespan is strongly influenced by genetics. Mutations in a single gene out of many thousand genes can increase lifespan in various model organisms including yeast, flies, worms and mice, and are associated with longevity in humans. Importantly, genes and interventions that increase lifespan in one species have been shown to be conserved across species (Friedman and Johnson, 1988; Holzenberger et al., 2003; Kenyon et al., 1993; Suh et al., 2008). Interestingly, these lifespan-extending genes have also been shown to be protective in animal models of neurodegenerative disease including AD (Cohen et al., 2006; Cohen et al., 2009; Freude et al., 2009; Killick et al., 2009), PD (Cooper et al., 2015; Knight et al., 2014), HD (Hsu et al., 2003; Jiang et al., 2012; Morley et al., 2002; Sadagurski et al., 2011), and ALS (Boccitto et al., 2012). This strongly suggests that targeting molecular pathways that modulate aging may be an effective strategy to treat neurodegenerative disease. Despite these exciting observations, it remains a challenge to translate genetic treatments to humans.
As an alternative, it may be possible to develop novel treatments for neurodegenerative diseases using compounds that modulate aging. In addition to identifying a plethora of genes that can affect longevity (https://genomics.sen...nce.info/genes/), aging research has also identified multiple compounds that extend lifespan in models organisms (http://genomics.senescence.info/drugs/ ). In this review, we examine the effects of five compounds that have been shown to modulate aging (metformin, resveratrol, rapamycin, N-acetyl-L-cysteine, and curcumin) in four neurodegenerative diseases (AD, PD, HD and ALS). We find that compounds that increase lifespan can be neuroprotective in models of neurodegenerative disease (Fig. 1), and thus may represent a novel treatment strategy for these disorders.

Fig. 1. Lifespan-extending compounds can be protective in neurodegenerative diseases. Five compounds that have been shown to increase lifespan in model organisms (metformin, resveratrol, rapamycin, N-acetyl cysteine, curcumin) have all been shown to have beneficial effects in four different neurodegenerative diseases (Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, amyotrophic lateral sclerosis).
2. Metformin
Metformin is a promising preventative treatment for age-associated diseases. Metformin is commonly used for treating Type 2 Diabetes Mellitus (T2DM), and retrospective studies discovered that metformin treatment of T2DM patients caused reduced incidents of age-associated diseases such as cardiovascular diseases (Campbell et al., 2017), cancers (Gandini et al., 2014; Wu et al., 2014), and neurodegenerative diseases (Cheng et al., 2014; Ng et al., 2014). In T2DM patients, metformin causes reduced glucose production in the liver, as well as increased insulin sensitivity in the peripheral tissues (Giannarelli et al., 2003). Metformin is delivered orally and disperses throughout the body to the liver, kidney, muscles, and the brain (Gormsen et al., 2016; Kulkarni et al., 2018; Labuzek et al., 2010), which may explain its widespread physiological effects. The specific molecular interactions of metformin are still unclear. However, metformin leads to activation of the highly conserved energy-sensing AMP-activated protein kinase (AMPK) pathway (Fullerton et al., 2013; Zhou et al., 2001). Metformin also independently activates mTORC1, which causes activation of AMPK through a lysosomal pathway (Kalender et al., 2010; Zhang et al., 2016). Activation of the AMPK pathway corrects energy imbalances by increasing lipid metabolism, increasing mitochondrial biogenesis, increasing autophagy, delaying cell cycle progression and decreasing protein production (Hardie et al., 2012). The AMPK pathway also modulates inflammation and inhibits the c-Jun N-terminal kinase (JNK) pathway (Chen et al., 2019; Hu et al., 2016). Therefore, metformin treatment regulates multiple pathways associated with aging.
2.1. Effect of metformin on lifespan
Metformin has mixed effects on lifespan in various model organisms (Table 1), but improves healthspan experimentally in murine models and is associated with decreases in age-related diseases in humans with T2DM. Metformin was first shown to extend lifespan in C. elegans (Onken and Driscoll, 2010), but, interestingly, this effect was due to metabolic changes in the bacterial food source, not the nematodes (Cabreiro et al., 2013). Subsequent studies were unable to demonstrate a beneficial effect of metformin on lifespan in Drosophila (Slack et al., 2012). In mice, metformin was shown to cause a small, but statistically significant, increase in lifespan (Martin-Montalvo et al., 2013). However, a larger study performed at multiple locations with genetically heterogenous mice failed to find a statistically significant increase in lifespan when animals were treated with metformin alone (Strong et al., 2016). Nonetheless, metformin exhibits a more clearly beneficial effect on the healthspan of mice (Feng et al., 2020; Martin-Montalvo et al., 2013). This is consistent with previous research showing that metformin improves cardiovascular function and cognition in aging mice (Campbell et al., 2017; UKPDS, 1998). In retrospective cohort studies, metformin was associated with extended lifespan of T2DM patients (Bannister et al., 2014; Campbell et al., 2017). Based on these promising results, a large randomized controlled study has been planned to determine if metformin affects lifespan and healthspan in healthy humans (Barzilai et al., 2016).
Table 1. Effect of compounds on lifespan in model organisms.
2.2. Metformin and Alzheimer’s disease
In the majority of studies reported, metformin is protective against dementia and AD in model organisms and in humans (Table 2). Treatment with metformin ameliorates phenotypic deficits in AD models in cell culture (Chen et al., 2016), C. elegans (Ahmad and Ebert, 2017), Drosophila (Niccoli et al., 2016), and mice (Chen et al., 2019; Farr et al., 2019; Ou et al., 2018). Metformin treatment after phenotypic onset improved behavioral phenotypes in APP/PS1 mice (Matthes et al., 2018) and in an STZ-induced AD rodent model (Nassar et al., 2018). In contrast, metformin treatment exacerbated motor and behavioral deficits in a P301S mutant human tau mouse model (Barini et al., 2016). Metformin treatment also increased tau phosphorylation in murine AD models expressing human ApoE3 or ApoE4 (Zhang et al., 2019). Interestingly, metformin still improved cognition in the ApoE3 mouse, but not the ApoE4 mice, suggesting that genetic differences can influence the efficacy of metformin in treating AD. Another cautionary note is that metformin can cause increased Aβ production, which is inhibited by insulin (Chen et al., 2009). In patients with T2DM, metformin treatment alone was associated with a decrease in the risk of dementia in multiple retrospective cohort studies (Bohlken et al., 2018; Cheng et al., 2014; Hsu et al., 2011; Orkaby et al., 2017; Shi et al., 2019). However, two studies did find that metformin treatment of T2DM patients was associated with an increased risk of developing AD (Imfeld et al., 2012; Kuan et al., 2017). Metformin has been proposed to be protective against AD by inhibiting the JNK pathway, causing suppression of cell death (Chen et al., 2016). It may also be protective through increasing glucose transport in neurons (Niccoli et al., 2016). While metformin has promising effects on AD models, more research needs to be done to determine why it has detrimental effects in certain systems.
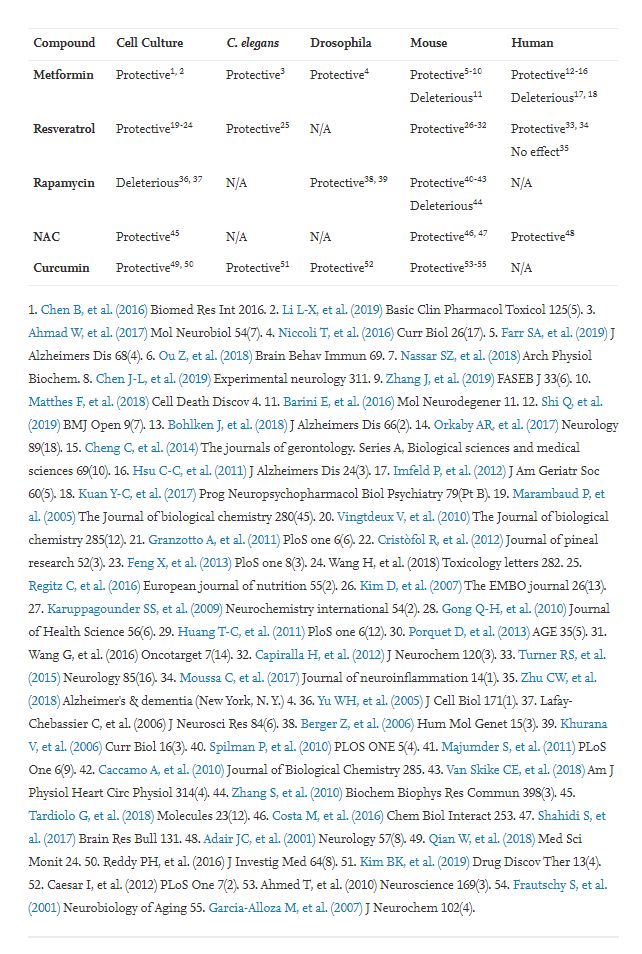
Table 2. Effect of compounds on Alzheimer’s disease.
.../...
.
Edited by Engadin, 04 July 2020 - 08:38 PM.













