I've been wondering about this myself and learned the following: (standard disclaimer applies: check my statements on your own, please correct me if I'm wrong)
- Trimethylglycine (TMG) isn't really a precursor to S-adenosyl-L-methionine (SAMe). TMG is a methyl donor in the conversion of homocysteine to methionine by betaine-homocysteine methyltransferase (BHMT). BHMT is not active in the brain.
Other important cofactors in the conversion of homocysteine to methionine are: methylcobalamin(B12) and folate.
Methylcobalamin is the other methyl donor in the conversion of homocysteine to methionine through methionine synthase. Methionine synthase uses 5-methyltetrahydrofolate(5MTHF) to donate a methyl group to cobalamin, creating methylcobalamin.
We get 5MTHF from:
folate -> dihydrofolate -> tetrahydrofolate -> Methylene-THF -> 5-methyltetrahydrofolate
- Methionine is converted to SAMe by methionine-adenosyl-transferase with magnesium (required), potassium (required), atp and water as cofactors.
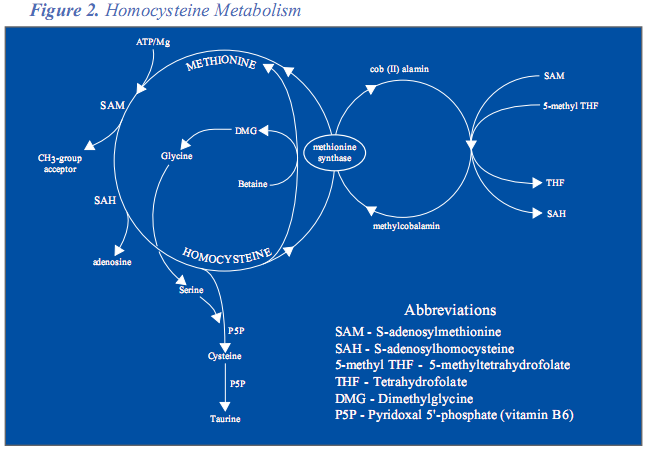
This
article provides a great more detail of all the above. It also summarizes everything in a visual manner, which I think is worth showing in the post:
I tried and failed to locate the oral bioavailability of l-methionine. I did find two studies that examined the relationship of oral methionine and the observed increase of homocysteine, which indicates that the oral methionine is being converted to SAMe, as:
methionine->SAMe->S-adenosylhomocysteine->homocysteine
The two studies are:
Hanratty CG, McGrath LT, McAuley DF, Young IS, Johnston GD. The effects of oral methionine and homocysteine on endothelial function. Heart. 2001 Mar;85(3):326-30.Fukagawa NK, Martin JM, Wurthmann A, Prue AH, Ebenstein D, O'Rourke B. Sex-related differences in methionine metabolism and plasma homocysteine concentrations. Am J Clin Nutr. 2000 Jul;72(1):22-9Both of these studies use a 100mg/kg human dose, which in a 60kg adult is 6 grams of l-methionine.
Based on all of this, my thoughts are:
- Assuming I don't have a methionine-adenosyl-transferase(MAT) deficiency of some sort, then I should be able to produce SAMe from normal dietary intake of methionine.
- By supplementing with TMG, methylcobalamin, folate and B6, I should be able to reduce my homocysteine and in turn increase methionine to ensure optimal levels of SAMe. I would prefer this approach rather than supplementing with l-methionine and risk increasing my homocysteine levels.
- If I do not observe any sort of mood enhancement from the previous supplementation, I may have to supplement with SAMe directly.
Topics for another post/ more research
- Something I found while researching SAMe was how non-academic texts, i.e. websites, categorically state that SAMe alleviates depression by contributing to the synthesis of serotonin and other monoamines (poor evidence for this). The academic texts (at least the several dozen I've read) are still quite uncertain about the exact mechanisms through which SAMe helps depression. If I have an opportunity, I'll put together everything I've found in a post or post in an appropriate existing topic.
- hypermethylation vs hypomethylation, in the epigenetic sense.
- While looking into all of this, I ran into the concept of dietary methionine restriction and its relation to an observed increase in life span, which I still don't understand completely. I really need to dig into that, considering it results in a reduction of SAMe levels in the body.
That's all I have.
Edited by Wulf, 20 August 2008 - 12:01 PM.






















































