All:
First, a lot of folks are speculating that the immunosuppressive effects of rapamycin are distinct from its suppression of mTOR. In fact, the two are directly mechanistically linked, through mTOR's effects on the proliferation of T-cells and the proliferation and activation of B-cells (6). So don't imagine that you can get one without the other, or that rapamycin's effects are simple antiinflammatory ones (as if the catch-all "antiinflammatory" were
simple ...). Moreover, it causes hypercholesterolemia: that may be an entirely acceptable tradeoff in a cancer patient or transplant recipient (or in a mouse, who doesn't face the risk of heart disease), but it's a lousy bet for an otherwise-healthy human, for whom CHD remains the number one killer.
Speaking of which:
And of course all this relates back to human beings, who don't seem so much to die from cancer (or at least I gather they don't), and certainly not from lymphoma in particular.
Don't know where you got that impression: cancer remains the number two cause of death in American
men and
women, and as the tables linked on those pages show, it's actually the number
one cause for several decades in midlife and early seniority in both genders -- ie, right around the sixty-year mark extrapolated from the rodent study.
Now:
There is a large group of multiple myeloma patients taking as much as 8 grams of turmeric daily, for over four years. It seems to be a viable treatment for the condition. Some side effects are reported HERE .
There are
thirty people in that trial, and we're hearing only the self-reported anecdotes from the minority of patients taking part in an online discussion forum after just a couple of years of taking the stuff, likely including at least a few folks on placebo; I wouldn't exactly call that a reliable data source. And, of course, people with a devastating disease like multiple myeloma are not exactly the best people in whom to test for subtle, slow-acting effects. Remember how long it took to definitively establish the problems with Rezulin and Vioxx; remember that this was after being used by literally thousands of patients, under rigorous monitoring, for many years, in
relatively healthy people. It was only after they got out into even wider use that the problems began to be clear.
“Do Not Use for Seven Years After FDA Approval” Drugs
For many years, we have warned patients not to use newly approved drugs unless they are one of the decided minority of new drugs with evidence that they provide a breakthrough beyond existing treatments. A study, involving Dr. Sidney Wolfe as one of the authors, provides clear evidence why this caution of waiting seven years is well founded. A total of 548 new chemical entities (drugs marketed for the first time in the United States) were approved in 1975–1999. By 1999, 45 drugs (8.2%) acquired one or more black-box warnings and 16 (2.9%) were withdrawn from the market. The estimated probability of acquiring a new black-box warning or being withdrawn from the market over a period of 25 years was 20%. Half of these black-box warning changes occurred within 7 years of drug introduction; half of the withdrawals occurred within 2 years. The article concluded that serious adverse drug reactions commonly emerge after FDA approval. The safety of new agents cannot be known with certainty until a drug has been on the market for many years.2 This study provides the basis for our “Seven-Year Rule” concerning newly marketed drugs that are not therapeutic breakthroughs.
Therefore, one way of protecting yourself without being deprived of new, breakthrough drugs, is to say no to using newly approved drugs unless they are in the small minority of such drugs with a significant therapeutic benefit.
On balance, it seems to me the risks from curcumin supplementation are low enough to outweigh the possible unknown negatives. Especially if one is over sixty.
The risks aren't low -- they're
unknown. And the
benefits are unknown, too: we have yet to see a lifespan study with
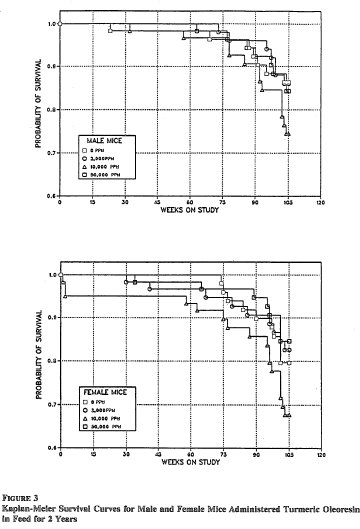
curcumin in normal, healthy rodents, and two-year toxicity and carcinogenicity studies at multiple doses in mice and rats showed no consistent or significant benefits. (1)
Let's remind ourselves of the slippery slope we're skating down, folks.
Rapamycin, a toxic immunosuppressant, has been shown
in a rodent study to extend lifespan when administered to old (not yet young) mice.
One of the things that rapamycin does is inhibit mTOR.
Curcumin,
in a test tube and in
mutant mice with cancer, has been found to inhibit mTOR at high dose.
We are
assuming that rapamycin will slow aging in humans the way that it appears to do in mice; on that assumption, we are
assuming that it will not kill us by toxic immunosuppression first; on those assumptions, we we are
assuming that it does so through mTOR, and not one of the other off-target effects of rapamycin; on those assumptions, we we are
assuming that the effects of curcumin on mTOR under highly abnormal conditions will also do occur in
normal, healthy organisms; on those assumptions, we we are
assuming that this will all occur in
humans; on those assumptions, we we are
assuming that the benefits of mTOR inhibition by rapamycin will also be exhibited by curcumin's (still uncertain!) effects on mTOR, even tho' we've already seen from the paper Niner posted (3) and in more detail from a recent review on efforts to come up with new 'tweaked' rapamycin analogs (4) that there are multiple ways to regulate the two enzyme isoforms and their up- and downstream targets, so that mTOR inhibition from rapamycin may not have hte same effects as the
possible "mTOR inhibition" by curcumin; and we are also
assuming that none of curcumin's zillion off-target effects ("including cell proliferation pathway (cyclin D1, c-myc), cell survival pathway (Bcl-2, Bcl-xL, cFLIP, XIAP, c-IAP1), caspase activation pathway (caspase-8, 3, 9), tumor suppressor pathway (p53, p21) death receptor pathway (DR4, DR5), mitochondrial pathways, and protein kinase pathway (JNK, Akt, and AMPK)", a wide variety of inflammatory markers, and the "GST enzyme activity [that] has been shown to be up- or down-regulated in rat tissues after oral consumption of curcumin, depending on the dose and route of administration" (2) -- ie, the fact that it's a very 'dirty' agent) won't outweigh these
purported benefits ...
Even though (again!) the 2-year toxicology studies on curcumin show no
clear benefits in normal mice or rats at all, at all.
Now, look. The people on Imminst are, with very few exceptions, relatively young, very healthy folks, with good lifestyles, relatively high socioeconomic status, etc. If you're an
average (let alone an unusually-health-conscious) 60-year-old, you have about thirty years of life expectancy left -- and if you're thirty, of course, you have many more. You'd be taking this stuff for
decades. I put it to you that there is no good reason to gamble your existing good health on what is at the moment an hypothesis-piled-on-hypothesis house of cards whose analog in Biblical scholarship is
The Holy Blood and the Holy Grail.
some good points by MR. I do agree with Maxwatt, however. There are a billion people in India eating curcumin in droves, which has only helped the country to show a lower level of alzheimers.
Hoo, boy. Prophets, I fear that your usually good instincts for the evidence were momentarily on vacation, here

.
First, "
traditional use" is an extremely unreliable basis for making safety or efficacy decisions. Imagine if the West had not latched upon tobacco, and it were just being latched upon by the supplement industry today. "Tobacco has been used in traditional Native American medicine for millennia before Columbus. Used in healing ceremonies, tobacco is treasured for its ability to energize, motivate, and lend a sense of clarity and focus to users. While an initial irritation can develop on first use, users quickly adjust to this healing crisis. No side-effects have been reported."
Second: turmeric is
5% curcuminoids. Suppose that an average Indian consumes one whole tablespoon of the stuff a day (a typical curry-type recipe might contain a
teaspoon of the stuff) -- that's 6.8 g turmeric, wich is 340 mg curcuminoids. It takes multi-gram doses of curcumin a day before it even starts to show up in your blood -- and even then, almost entirely as glucuronidated and sulfated liver-enzyme metabolites! I put it to you that there is really no analogy from its presence in the Indian diet, even if that were relevant data -- which it's not:
Third, to jump from "this
entire nation eats a lot of X and gets less disease Y compared to this other
entire nation" is
cross-cultural junk science.
And
fourth,
even if cross-cultural comparisons were a reasonable source of health information (and they're not!), the belief that Indians (and people in many other developing nations) have lower incidence of dementia is actually outdated, based in large part in the lack of adaptation of the DSM-IV criteria to the local culture: using a system designed for international use, the standardized prevalence adjusted for age, sex, and education is 8.2-8.7% (similar to Western Europe), not the 0.8-2.7% previously reported.(5)
Given that both CR and Rapamycin seem to work through inhibiting mTor, I don't see the harm in speculating on the mechanism involved.
Speculating about the mechanism is harmless; indeed, it's a necessary part of the scientific process. The next step from speculation is testing that speculation out -- in
rodents, not in yourself! -- and with (at least initially) highly-controlled conditions, including highly-specific agents, not a molecular 'shotgun' like curcumin.
What I consider an "inflammatory response" is basically anything that involves the body responding to ROS, not necessarily a persistent condition of arthritis treated with aspirin. Running outside produces ROS and the body responds to it. If CR reduces MitROS output, such that the body sustains less damage. If Rapamycin retards protein synthesis and the body's response to ROS (even if it occurs), then there are some mechanistic parallels here, at the very least.
These are really very different phenomena. The principle problem with mtROS is (most likely) that they cause large deletion mutations in mitochondrial DNA, not their direct effects on the rest of cells and tissues. Those other effects -- or the body's inflammatory responses to them -- are quite another matter. And chronically modulating inflammatory responses with rapamycin or curcumin would be very closely analogous to doing so with chronic inflammation, since mtROS are being puked out all the time, and at rising rates with age
So the ITP showed that rapamycin extends lifespan of lab mice. Many here are talking about curcumin, because it also inhibits mTOR, and is a priori less dangerous for humans. Curcumin is on the list of things to be tested by the ITP: http://www.nia.nih.g...dsInTesting.htm
Yes. So let's at least wait a few years for the ITP to give us some lifespan studies before self-experimenting, OK? Remember the null effects and occasional disasters already encountered with innocent-looking
essential nutrients like folic acid, selenium, and sundry "antioxidants."
Look, folks: we have
decades -- and we're in this game for
millennia.
We have time on our side. We are working toward an ageless future of unlimited youthful lifespans, with life expectancies in the multiples of centuries -- let's start thinking like the kinds of people we must become. For starters, let's learn some freakin'
patience, for crying out loud

!
-Michael
1: Ravindran J, Prasad S, Aggarwal BB. Curcumin and Cancer Cells: How Many Ways Can Curry Kill Tumor Cells Selectively? AAPS J. 2009 Jul 10. [Epub ahead of print] PubMed PMID: 19590964.
3. Thoreen CC, Kang SA, Chang JW, Liu Q, Zhang J, Gao Y, Reichling LJ, Sim T, Sabatini DM, Gray NS.
An ATP-competitive mammalian target of rapamycin inhibitor reveals rapamycin-resistant functions of mTORC1. J Biol Chem. 2009 Mar 20;284(12):8023-32. Epub 2009 Jan 15. PubMed PMID: 19150980; PubMed Central PMCID: PMC2658096.
3. National Toxicology Program.
NTP Toxicology and Carcinogenesis Studies of Turmeric Oleoresin (CAS No. 8024-37-1) (Major Component 79%-85% Curcumin, CAS No. 458-37-7) in F344/N Rats and B6C3F1 Mice (Feed Studies). Natl Toxicol Program Tech Rep Ser. 1993 Aug;427:1-275. PubMed PMID: 12616304.
4. Abraham RT, Gibbons JJ.
The mammalian target of rapamycin signaling pathway: twists and turns in the road to cancer therapy. Clin Cancer Res. 2007 Jun 1;13(11):3109-14. Review. PubMed PMID: 17545512.
5. Llibre Rodriguez JJ, Ferri CP, Acosta D, Guerra M, Huang Y, Jacob KS, Krishnamoorthy ES, Salas A, Sosa AL, Acosta I, Dewey ME, Gaona C, Jotheeswaran AT, Li S, Rodriguez D, Rodriguez G, Kumar PS, Valhuerdi A, Prince M; 10/66 Dementia Research Group. Prevalence of dementia in Latin America, India, and China: a population-based cross-sectional survey. Lancet. 2008 Aug 9;372(9637):464-74. Epub 2008 Jul 25. PubMed PMID: 18657855.
6.Maria Z. Siemionow. Tissue surgery. ISBN 1852339705. Springer, 2006.
Pg 18.
Edited by Michael, 13 July 2009 - 05:59 PM.



















































