All:
I hope to post more on various issues later ... meanwhile:
- First, a big shout-out for Kismet for doing high-quality analysis on this thread!
Second: I'm sure those who've even perused the abstract will've noticed this very important fact, but for those who haven't and those who haven't yet dug further:
In a separate study, rapamycin fed to mice beginning at 270 days of age also increased survival in both males and females, based on an interim analysis conducted near the median survival point. …
At the time of analysis, 51% of the females and 68% of the males had died, and a stratified log-rank test showed significantly lower mortality risk in the rapamycin-treated mice compared to controls, pooling across the three test sites (P=0.0002 for males and P<0.0001 for females). When each site was evaluated separately, the beneficial effect of rapamycin for females was significant at each site (P,0.005); for males, the effect was significant (P<0.025) at UM and UT, but not at TJL. [MR: The 3 labs, unfortunately, used different diets early on, both between labs and (for UM and UT) between control and treated males, and this study and esp the previous report suggest that this affected later LS in the males; here, "We thus cannot rule out the possibility that improved survival among males in the rapamycin group, at UT and at UM, might reflect differences in nutritional or health status between control and rapamycin groups before 600 days, rather than solely the effects of rapamycin. Notably, the significant benefits of rapamycin on male (and female) survival at TJL could not have been affected by diet before drug administration, because at TJL both control and rapamycin-fed mice received the same chow (Purina 5LG6) throughout this period. "] Rapamycin seems to reduce mid-life mortality risk when started at 270 days of age, but additional data are needed to provide an accurate estimate of effect size, and to evaluate effects on maximal longevity.
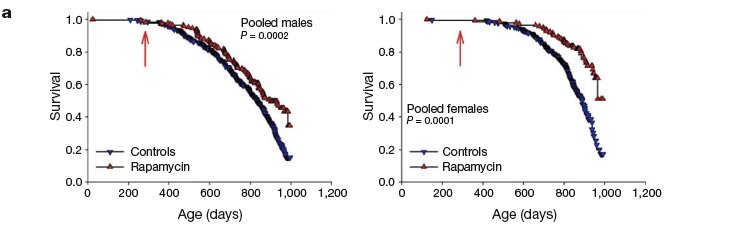
Survival plots for male and female mice, comparing control mice to rapamycin-treated mice ... from 270 days of age. Because at the time of the interim analysis all live mice were between 800 and 995 days of age, we have only limited information about the shape of the survival curve at ages above 900 days, and the apparent change in slope at the oldest ages (.990 days) reflects this experimental uncertainty.
That certainly
looks like there's going to be an extension of max LS -- but then, the same was true at the median point for NGDA in the first round ...
Another happy thing: even the stated data for mean and max LS extension for the late-onset animals likely slightly downplays the power of the result, as at the time of analysis not
all of the animals had died:
We analysed the data set as of 1 February 2009, with 2% (38 of 1,901) of mice still alive. … Summing across the three sites, 4.8%of the female control mice were alive at these ages, compared with 21.5% of the rapamycin-treated females (P<0.0001). For males, the corresponding values were 5.9% of controls and 20.2% of rapamycin-treatedmice (P<0.0001). The site-specific calculations documented a significant effect on females at both TJL (P=0.0006) and UM (P=0.0001); for males, we noted a significant effect at both TJL (P=0.008) and UT (P=0.0001), with a marginal effect at UM (P=0.07). Rapamycin feeding initiated at 600 days of age thus leads to a significant increase in maximal lifespan.
To test if the spectrum of lesions was altered by dietary rapamycin, complete necropsies were conducted on 31 control and 40 rapamycinfed mice that were either found dead or killed when moribund (details in Supplementary Table 2). Although rapamycin postpones death, it did not change the distribution of presumptive causes of death.
This, I think, largely mitigates against the concern that it's only a cancer-preventive, since it doesn't appear that it
was preventive. However, as Kismet notes, (a) there did actually look to be an
increase in lymphoma in the treated group, and (b)they don't appear to give enough info to say whether there was a difference in
age-specific incidence rates, or if more animals died of cancer simply because of a shift in causes of age-related death -- or, for that matter, if more treated animals died
with, but not
of, a higher burden of slow-growing, nonfatal tumors.
Speculation..all speculation
Too much, in this thread, I fear. Folks, I implore you as friends and life extensionists
not to fall prey to the temptation to leap from a
possible mechanism to supplementation based on that mechanism (especially not
in vitro!), especially not with very 'shotgun' supplements like curcumin, and especially not on the basis of the in vitro effects of those supplements. There are plenty of drugs that lower cholesterol or blood pressure, but kill you dead for other reasons.
































 LongeCity
LongeCity














