






























Any news regarding
 LongeCity
LongeCityAdvocacy & Research for Unlimited Lifespans

 4 votes
4 votes

Posted 21 November 2013 - 05:40 AM
Edited by YoungS, 21 November 2013 - 05:41 AM.


Posted 21 November 2013 - 07:43 AM
I'm interested. Could you check and see if Nefiracetam works for any of your positive symptoms or IDRA-21? Just out of curiosity.I'm going to be in a phase III trial of EVP-6124 (alpha-7 nicotinic partial agonist) in schizophrenics within a couple of months!
http://clinicaltrial...how/NCT01714713
http://www.internalm...38e782e8587b6d3
http://www.envivopha...-item.php?id=45
http://www.envivopha...e-nicotinic.php
http://www.envivopha...-item.php?id=32
I'll maybe share my experiences when the trial starts..
Posted 21 November 2013 - 03:10 PM

Edited by YoungS, 21 November 2013 - 04:06 PM.

Posted 06 October 2016 - 01:12 PM
Eur J Pharmacol. 2013 Jan 5;698(1-3):228-34.
Sub-anesthetic concentrations of (R,S)-ketamine metabolites inhibit acetylcholine-evoked currents in α7 nicotinic acetylcholine receptors.
Moaddel R1, Abdrakhmanova G, Kozak J, et al.
Abstract
The effect of the (R,S)-ketamine metabolites (R,S)-norketamine, (R,S)-dehydronorketamine, (2S,6S)-hydroxynorketamine and (2R,6R)-hydroxynorketamine on the activity of α7 and α3β4 neuronal nicotinic acetylcholine receptors was investigated using patch-clamp techniques. The data indicated that (R,S)-dehydronorketamine inhibited acetylcholine-evoked currents in α7-nicotinic acetylcholine receptor, IC(50) = 55 ± 6 nM, and that (2S,6S)-hydroxynorketamine, (2R,6R)-hydroxynorketamine and (R,S)-norketamine also inhibited α7-nicotinic acetylcholine receptor function at concentrations ≤ 1 μM, while (R,S)-ketamine was inactive at these concentrations. The inhibitory effect of (R,S)-dehydronorketamine was voltage-independent and the compound did not competitively displace selective α7-nicotinic acetylcholine receptor ligands [(125)I]-α-bungarotoxin and [(3)H]-epibatidine indicating that (R,S)-dehydronorketamine is a negative allosteric modulator of the α7-nicotinic acetylcholine receptor. (R,S)-Ketamine and (R,S)-norketamine inhibited (S)-nicotine-induced whole-cell currents in cells expressing α3β4-nicotinic acetylcholine receptor, IC(50) 3.1 and 9.1 μM, respectively, while (R,S)-dehydronorketamine, (2S,6S)-hydroxynorketamine and (2R,6R)-hydroxynorketamine were weak inhibitors, IC(50) >100 μM. The binding affinities of (R,S)-dehydronorketamine, (2S,6S)-hydroxynorketamine and (2R,6R)-hydroxynorketamine at the NMDA receptor were also determined using rat brain membranes and the selective NMDA receptor antagonist [(3)H]-MK-801. The calculated K(i) values were 38.95 μM for (S)-dehydronorketamine, 21.19 μM for (2S,6S)-hydroxynorketamine and>100 μM for (2R,6R)-hydroxynorketamine. The results suggest that the inhibitory activity of ketamine metabolites at the α7-nicotinic acetylcholine receptor may contribute to the clinical effect of the drug.
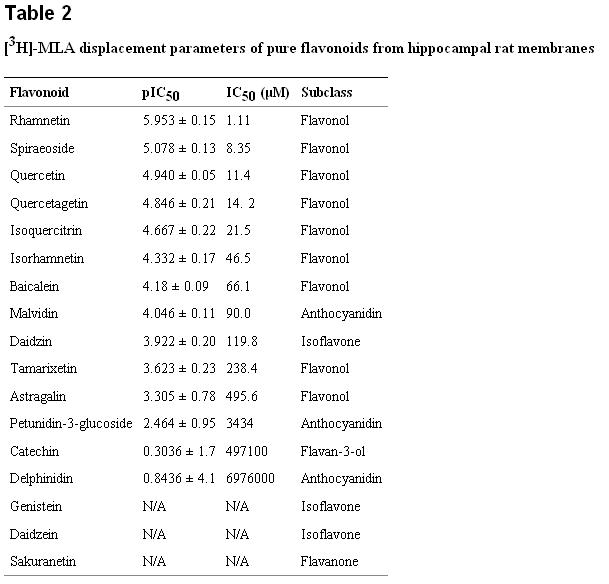
from a 2014 study, flavonoid affinities.
"... methyllycaconitine (MLA) is a relatively selective ligand for the alpha7 nAChR subtype that is isolated from the seeds of Delphinium brownii, a North American wildflower [19]."
Nicotinic α7 Receptors as a New Target for Treatment of Cannabis Abuse
Marcello Solinas, Maria Scherma, Liana Fattore
Abstract
Increasing use of cannabis makes the search for medications to reduce cannabis abuse extremely important. Here, we show that homomeric α7 nicotinic receptors are novel molecular entities that could be targeted in the development of new drugs for the treatment of cannabis dependence. In rats, systemic administration of the selective α7 nicotinic acetylcholine receptor antagonist methyllycaconitine (MLA), but not the selective heteromeric non-α7 nicotinic acetylcholine receptor antagonist dihydrobetaerythroidine, (1) antagonized the discriminative effects of δ-9-tetrahydrocannabinol (THC), the main active ingredient in cannabis, (2) reduced intravenous self-administration of the synthetic cannabinoid CB1 receptor agonist WIN55,212-2 [®-(+)-[2,3-dihydro-5-methyl-3[(4-morpholinyl)methyl]pyrrolo[1,2,3-de]-1,4-benzoxazinyl]-(1-naphthalenyl)methanone, mesylate salt], and (3) decreased THC-induced dopamine elevations in the shell of the nucleus accumbens. Altogether, our results indicate that blockade of α7 nicotinic receptors reverses abuse-related behavioral and neurochemical effects of cannabinoids. Importantly, MLA reversed the effects of cannabinoids at doses that did not produce depressant or toxic effects, further pointing to α7 nicotinic antagonists as potentially useful agents in the treatment of cannabis abuse in humans.
Mol Cells. 2010 Sep;30(3):245-53.
Quercetin enhances human α7 nicotinic acetylcholine receptor-mediated ion current through interactions with Ca(2+) binding sites.
Lee BH1, Choi SH, Shin TJ, et al.
Abstract
The flavonoid quercetin is a low molecular weight substance found in fruits and vegetables. Aside from its anti-oxidative effect, quercetin, like other flavonoids, has a wide range of neuropharmacological actions. The α7 nicotinic acetylcholine receptor (α7 nAChR) has a Ca(2+)-binding site, is highly permeable to the Ca(2+) ion, and plays important roles in Ca(2+)-related normal brain functions. Dysfunctions of α7 nAChR are associated with a variety of neurological disorders. In the present study, we investigated the effects of quercetin on the ACh-induced inward peak current (I(ACh)) in Xenopus oocytes that heterologously express human α7 nAChR. I(ACh) was measured with the two-electrode voltage clamp technique. In oocytes injected with α7 nAChR cRNA, the effects of the co-application of quercetin on I(ACh) were concentration-dependent and reversible. The ED(50) was 36.1 + 6.1 μM. Quercetin-mediated enhancement of I(ACh) caused more potentiation when quercetin was pre-applied. The degree of I(ACh) potentiation by quercetin pre-application was time-dependent and saturated after 1 min. Quercetin-mediated I(ACh) enhancement was not affected by ACh concentration and was voltage-independent. However, quercetin-mediated I(ACh) enhancement was dependent on extracellular Ca(2+) concentrations and was specific to the Ca(2+) ion, since the removal of extracellular Ca(2+) or the addition of Ba(2+) instead of Ca(2+) greatly diminished quercetin enhancement of I(ACh). The mutation of Glu195 to Gln195, in the Ca(2+)-binding site, almost completely diminished quercetin-mediated I(ACh) enhancement. These results indicate that quercetin-mediated I(ACh) enhancement human α7 nAChR heterologously expressed in Xenopus oocytes could be achieved through interactions with the Ca(2+)-binding site of the receptor.
Fitoterapia. 2014 Oct; 98: 11–21.
A nicotinic receptor-mediated anti-inflammatory effect of the flavonoid rhamnetin in BV2 microgliaJoseph A. Lutz,aManish Kulshrestha,bDennis T. Rogers,c and John M. Littletond,*
AbstractThe alpha7 nicotinic acetylcholine receptor (nAChR) is a potential target in neuroinflammation. Screening a plant extract library identified Solidago nemoralis as containing methyl-quercetin derivatives that are relatively selective ligands for the alpha7 nAChR. Flavonoids are not known for this activity, so we screened a small library of pure flavonoids to confirm our findings. Some flavonoids, e.g. rhamnetin, displaced a selective alpha7 nAChR radioligand from rat brain membranes whereas similar structures e.g. sakuranetin, did not. To evaluate the contribution of this putative nAChR activity to the known anti-inflammatory properties of these flavonoids, we compared their effects on lipopolysaccharide induced release of inflammatory mediators from BV2 microglia. Both rhamnetin and sakuranetin reduced mediator release, but differed in potency (rhamnetin>sakuranetin) and the Hill slope of their concentration response curves. For rhamnetin the Hill coefficient was >3.0 whereas for sakuranetin the coefficient was 1.0, suggesting that effects of rhamnetin are mediated through more than one mechanism, whereas sakuranetin has a single mechanism. nACHR antagonists decreased the Hill coefficient for rhamnetin toward unity, which suggests that a nAChR-mediated mechanism contributes cooperatively to its overall anti-inflammatory effect. In contrast nAChR antagonists had no effect on the potency or Hill coefficient for sakuranetin, but a concentration of nicotine (1μM) that had no effect alone, significantly increased the Hill coefficient of this flavonoid. In conclusion, the anti-inflammatory effects of rhamnetin benefit cooperatively from a nAChR-mediated mechanism. This action, together with potent free radical scavenging activity, suggests that flavonoids with alpha7 nAChR activity have therapeutic potential in neuroinflammatory conditions.
 mla alpha7.jpg 51.44KB
0 downloads
mla alpha7.jpg 51.44KB
0 downloads
Edited by gamesguru, 06 October 2016 - 01:30 PM.

Posted 06 October 2016 - 01:26 PM
Aren't some nicotinic receptors a rare example of when agonism actually results in upregulation - and so the obvious question is does this apply to the alpha 7s?
6 years later, and I THINK we may finally have the answer to this... YES! Yes, it does.
In the Borderline-thread we've been searching with headbeams after compounds which affect Alpha-7, since Alpha-7-modulation shows IMMENSE promise in the treatment of this, the most VILE of all neuropsychiatric diseases - and as it turns out... people with mood-disorders actually seem to become MORE unstable when given Alpha-7-agonists...!
The conclusion we have drawn then, is that antagonism is more preferred.
Borderliners also have an immensely, NATURALLY enhanced cholinergic activity, doubtlessly this has something to do with it...
So, you have now strengthened my resolve: only by antagonising the Alpha-7-receptor to an UNPARALLELLED degree, to the point of vegetizing the Borderliners, can their emotional turmoil finally be CHAINED - they will be less snappy in the thinking department, but they will instead gain... a personality. Interests. Self-esteem.
IMHO, when you are as diseased as they are, it's a decent trade-off.
Posted 06 October 2016 - 01:35 PM
I'm late to this party, but just wanted to say that plain old Choline is a selective a7 agonist.
Wait... WHAT?!!
I'm not sure if you're aware of this, but a majority of Borderliners appear to have a genetic mutation causing overmethylation of choline, causing their levels to rise sky-high.
It's also been concluded that their issues are neuroanatomically connected to deformities in the prefrontal cortex and the amygdala.
Their issues bear a FRIGHTENING similarity to obscenely intrusive signalling from the amygdala, not properly sorted by the PFC - leading to rash and illogical, overly emotional behaviour.
If what you're saying is true...
Choline is an alpha-7-selective agonist...
They have massive amounts of choline...
Their amygdala is going haywire with signalling...
The signalling in and out of the amygdala is controlled by the alpha-7-receptors...
Well.
I suppose all borderliners should probably cut all eggs out of their diet, then?
Posted 06 October 2016 - 11:31 PM
eggs? naww dawwwg, cos you'd also havta get off the peanuts, the grains.. the meats (especially organ meats), spinach and beets. but ya can't be doing that, lad. so why not poke a lotta smot n raise dat acetylcholine turnover instead? bring on teh m0re logical replies
Stinky is right about the connection to Borderline Personality. He arrived at this conclusion with a little help from yours truly. But that's beside the point, because the way to get things done is not to care who gets credit for doing them. Since dopamine is also also involved[1], [2], [3], [4](perhaps to the same extent as serotonin and glutamate), and acetylcholine kind of works against dopamine, the idea also makes sense.
... giving patients with BPD a chemical that increases acetylcholine in the brain producers significantly more depressive symptoms than giving this chemical to patients who do not have BPD.
Posted 27 October 2016 - 10:09 PM
Aren't some nicotinic receptors a rare example of when agonism actually results in upregulation - and so the obvious question is does this apply to the alpha 7s?
6 years later, and I THINK we may finally have the answer to this... YES! Yes, it does.
In the Borderline-thread we've been searching with headbeams after compounds which affect Alpha-7, since Alpha-7-modulation shows IMMENSE promise in the treatment of this, the most VILE of all neuropsychiatric diseases - and as it turns out... people with mood-disorders actually seem to become MORE unstable when given Alpha-7-agonists...!
The conclusion we have drawn then, is that antagonism is more preferred.
Borderliners also have an immensely, NATURALLY enhanced cholinergic activity, doubtlessly this has something to do with it...
So, you have now strengthened my resolve: only by antagonising the Alpha-7-receptor to an UNPARALLELLED degree, to the point of vegetizing the Borderliners, can their emotional turmoil finally be CHAINED - they will be less snappy in the thinking department, but they will instead gain... a personality. Interests. Self-esteem.
IMHO, when you are as diseased as they are, it's a decent trade-off.
Your post made me smile. For the record, the closest you'll get to a selective a7 antagonist is memantine. Personally it didn't do much for me. Which is understandable given that it isn't used for neuropsychiatric problems like BPD.
However Quetiapine did work quite well, and I believe this does have intrinsic anti-cholinergic activity - whether that's related to its efficacy, I have no idea.
This is speculation on my part, but for some people, it may be worth supplementing Inositol. As Inositol and Choline are typically employed together, my guess is that they oppose each other.
I do remember reading that manic people typically have low levels of choline, yet high levels inositol (of which lithium reverses). Conversely, there's a lot of emerging evidence that depressed people are hyper-responsive to acetylcholine. Whether the muscarinic or the nicotinic receptors are to blame, I can't be sure at this point.

Posted 28 October 2016 - 01:42 AM
I think there might be a bunch of sleepiness or cognition impairing proteins that naturally circulate at normal humans. immunizing against these could then be measured as to their effectiveness as nootropics (smart drugs) or fatigue reducing drugs.
Ten minutes of looking at Pubmed [links] suggest two antibodies that could reduce fatigue and amplify cognition in normal people. Antibodies to (Serum anti-aquaporin 4 (AQP4) antibody), also the FDA approved antibody drug Natalizumab are published as causing cognitive or energetic recovery in abnormal persons. I recently read that reducing kynurenic acid production, knocking out the production of kynurenine aminotransferase II causes nicotine acetylcholine receptors to be more active. So immunizing against the cytokines that produce kynurenic acid could cause cause greater intelligence. [link]
Noting that some FDA approved antibody drugs reduce beta amyloid plaques, (that is, they are active at the brain) if they could find any naturally occurring NGF (Nerve growth Factor) absorbing proteins, immunizing against those absorbers might cause greater NGF at the brain, increasing intelligence.
There might be dozens of normal proteins that slightly impair normal cognition, so finding out what these are then immunizing against them (possibly with an oral vaccine) would produce a smart drug effective at one dose, that might last a lifetime!
An immunization to make people smarter http://www.halfbaker...eople_20smarter
Posted 29 October 2016 - 12:05 AM
Your post made me smile. For the record, the closest you'll get to a selective a7 antagonist is memantine. Personally it didn't do much for me. Which is understandable given that it isn't used for neuropsychiatric problems like BPD.
However Quetiapine did work quite well, and I believe this does have intrinsic anti-cholinergic activity - whether that's related to its efficacy, I have no idea.
This is speculation on my part, but for some people, it may be worth supplementing Inositol. As Inositol and Choline are typically employed together, my guess is that they oppose each other.
I do remember reading that manic people typically have low levels of choline, yet high levels inositol (of which lithium reverses). Conversely, there's a lot of emerging evidence that depressed people are hyper-responsive to acetylcholine. Whether the muscarinic or the nicotinic receptors are to blame, I can't be sure at this point.
Sad to hear it didn't work - but the Alpha-7-antagonism is pretty weak with Memantine. (glad to hear you're more stable with other meds though!)
There IS however another (weak) NMDA-antagonist with a much, MUCH stronger Alpha-7-effect these days...! : ) Recently discovered and refined:
HYDROXYNORKETAMINE!
https://en.wikipedia...roxynorketamine
I'm actually thinking of making a group-buy on that one... And then chase down my ex, chloroform her, shave off all of her hair, mix HNK with DMSO and then paint her entire scalp! It should have quite the effect then.
(oh, and then I'll ask her to marry me - as her glorious saviour... Ahh... such delirious dreams!)
eggs? naww dawwwg, cos you'd also havta get off the peanuts, the grains.. the meats (especially organ meats), spinach and beets. but ya can't be doing that, lad. so why not poke a lotta smot n raise dat acetylcholine turnover instead? bring on teh m0re logical replies
Stinky is right about the connection to Borderline Personality. He arrived at this conclusion with a little help from yours truly. But that's beside the point, because the way to get things done is not to care who gets credit for doing them. Since dopamine is also also involved[1], [2], [3], [4](perhaps to the same extent as serotonin and glutamate), and acetylcholine kind of works against dopamine, the idea also makes sense.
... giving patients with BPD a chemical that increases acetylcholine in the brain producers significantly more depressive symptoms than giving this chemical to patients who do not have BPD.
Lol! Yeah, ok, you're right - they need to lay off a LOT of different foods. ^^ Anyways, you're also right that YOU helped me reach this conclusion! = ) You, Jack and Devin are all part of the discovery - you should all have a credit in the mini-paper I'm working on.
With me as the sovereign leader of course. 
I think there might be a bunch of sleepiness or cognition impairing proteins that naturally circulate at normal humans. immunizing against these could then be measured as to their effectiveness as nootropics (smart drugs) or fatigue reducing drugs.
Ten minutes of looking at Pubmed [links] suggest two antibodies that could reduce fatigue and amplify cognition in normal people. Antibodies to (Serum anti-aquaporin 4 (AQP4) antibody), also the FDA approved antibody drug Natalizumab are published as causing cognitive or energetic recovery in abnormal persons. I recently read that reducing kynurenic acid production, knocking out the production of kynurenine aminotransferase II causes nicotine acetylcholine receptors to be more active. So immunizing against the cytokines that produce kynurenic acid could cause cause greater intelligence. [link]
Noting that some FDA approved antibody drugs reduce beta amyloid plaques, (that is, they are active at the brain) if they could find any naturally occurring NGF (Nerve growth Factor) absorbing proteins, immunizing against those absorbers might cause greater NGF at the brain, increasing intelligence.
There might be dozens of normal proteins that slightly impair normal cognition, so finding out what these are then immunizing against them (possibly with an oral vaccine) would produce a smart drug effective at one dose, that might last a lifetime!
An immunization to make people smarter http://www.halfbaker...eople_20smarter
Hmm! Now that's a pretty clever idea, friend!
I've never even considered anything like that... using immunisation to enhance cognitive functions. I'm a little bit iffy on it though, because in some people I'm going to guess that it might be unbenefficial to immunize against all of these proteins - I'm thinking some of them serve a purpose, depending on your internal biochemistry - so perhaps not a magic bullet for everyone.
Posted 26 August 2017 - 02:25 PM
I'm going to be in a phase III trial of EVP-6124 (alpha-7 nicotinic partial agonist) in schizophrenics within a couple of months!
http://clinicaltrial...how/NCT01714713
http://www.internalm...38e782e8587b6d3
http://www.envivopha...-item.php?id=45
http://www.envivopha...e-nicotinic.php
http://www.envivopha...-item.php?id=32
I'll maybe share my experiences when the trial starts..
You never reported back on this.
WHY?
It should be helpful for exactly the issue you have, but nothing ever came of it? What's up here, man? Were you disqualified from the study?
Sad to hear it didn't work - but the Alpha-7-antagonism is pretty weak with Memantine.
I don't remember Memantine being a weak one. Bupropion is.
All right, I gotta' admit - I made an assumption here. Wanna' know why? 'Cause I can't find jack sh*t regarding the affinity of Memantine for Alpha-7! Nor if it is truly an antagonist, or a partial agonist.
Nothing.
If you could supply the affinity-data so we can have a closer look, then that would be lovely.
The affinity-data for Bupropion is known though, and it is indeed pitifully weak.
Edited by Stinkorninjor, 26 August 2017 - 02:28 PM.
Posted 26 August 2017 - 06:12 PM
I'm going to be in a phase III trial of EVP-6124 (alpha-7 nicotinic partial agonist) in schizophrenics within a couple of months!
http://clinicaltrial...how/NCT01714713
http://www.internalm...38e782e8587b6d3
http://www.envivopha...-item.php?id=45
http://www.envivopha...e-nicotinic.php
http://www.envivopha...-item.php?id=32
I'll maybe share my experiences when the trial starts..
You never reported back on this.
WHY?
It should be helpful for exactly the issue you have, but nothing ever came of it? What's up here, man? Were you disqualified from the study?
The study never got off the ground/started because the funding was not granted to the local hospital by the medicine authority. We'll never know if it might have worked since the company (ENVIVO) that would bring it to the market got bankrupted after phase III trials failed in schizophrenia and because some serious adverse effects in phase III trials for Alzheimer disease.
But even though it failed, I think this is just another late stage drug that would have helped a majority of schizophrenics. (And, yeah, maybe I'm one of those, but I'll never know I guess)
Posted 26 August 2017 - 06:52 PM
I'm going to be in a phase III trial of EVP-6124 (alpha-7 nicotinic partial agonist) in schizophrenics within a couple of months!
http://clinicaltrial...how/NCT01714713
http://www.internalm...38e782e8587b6d3
http://www.envivopha...-item.php?id=45
http://www.envivopha...e-nicotinic.php
http://www.envivopha...-item.php?id=32
I'll maybe share my experiences when the trial starts..
You never reported back on this.
WHY?
It should be helpful for exactly the issue you have, but nothing ever came of it? What's up here, man? Were you disqualified from the study?
The study never got off the ground/started because the funding was not granted to the local hospital by the medicine authority. We'll never know if it might have worked since the company (ENVIVO) that would bring it to the market got bankrupted after phase III trials failed in schizophrenia and because some serious adverse effects in phase III trials for Alzheimer disease.
But even though it failed, I think this is just another late stage drug that would have helped a majority of schizophrenics. (And, yeah, maybe I'm one of those, but I'll never know I guess)
Sad to hear that mate, but, there is always 5ht3-antagonists for you - they at least have a known and well-tested side-effects profile.
Don't necessarily give up on this though, because tht.co put one of these compounds to market, did they not? IDRA-21...? Can't quite recall the name right now...
Anyways, what were the serious adverse effects in Alzheimers? THAT part actually sounds scary! : O Could this side-effect be shared with other Alpha-7-agonistic compounds?
Posted 26 August 2017 - 08:03 PM
I'm going to be in a phase III trial of EVP-6124 (alpha-7 nicotinic partial agonist) in schizophrenics within a couple of months!
http://clinicaltrial...how/NCT01714713
http://www.internalm...38e782e8587b6d3
http://www.envivopha...-item.php?id=45
http://www.envivopha...e-nicotinic.php
http://www.envivopha...-item.php?id=32
I'll maybe share my experiences when the trial starts..
You never reported back on this.
WHY?
It should be helpful for exactly the issue you have, but nothing ever came of it? What's up here, man? Were you disqualified from the study?
The study never got off the ground/started because the funding was not granted to the local hospital by the medicine authority. We'll never know if it might have worked since the company (ENVIVO) that would bring it to the market got bankrupted after phase III trials failed in schizophrenia and because some serious adverse effects in phase III trials for Alzheimer disease.
But even though it failed, I think this is just another late stage drug that would have helped a majority of schizophrenics. (And, yeah, maybe I'm one of those, but I'll never know I guess)
Sad to hear that mate, but, there is always 5ht3-antagonists for you - they at least have a known and well-tested side-effects profile.
Don't necessarily give up on this though, because tht.co put one of these compounds to market, did they not? IDRA-21...? Can't quite recall the name right now...
Anyways, what were the serious adverse effects in Alzheimers? THAT part actually sounds scary! : O Could this side-effect be shared with other Alpha-7-agonistic compounds?
Which one does tht.co have on the market?
While the EVP phase III trial in schizophrenia still continued the FDA put the phase III Alzheimer trial to hold due to some severe gastrointestinal events. After the schizophrenia trial failed, they also terminated the trial for Alzheimer's (although they were allowed to continue).









0 members, 17 guests, 0 anonymous users


Community Forum Software by IP.Board
Licensed to: ImmInst.org


