And now for something completely different than anything I've written about The Inflammatory Reflex in the past...
The Inflammatory Reflex is a reflex in a way comparable to other sensory and motor reflexes. Among the most often cited examples is the Hand-on-a-Burning Stove example.
Put your finger or hand on a hot surface and almost immediately, there is a response to pull it away. The Sensory (aka, Afferent) arm of the Reflex senses the extreme heat and a signal proceeds up this Sensory Neuron to an InterNeuron which, first, processes the signal, and then sends the Pull-It-Away signal via Motor (aka, Efferent) Neurons, and the arm is pulled away. See the figure that illustrates the point.
Now, up to this time, I've only been posting about the Motor (Efferent) arm of The Inflammatory Reflex. But there is a Sensory (Afferent) arm and Kevin Tracey and his colleagues have recently published a study about the Afferent arm.
I summarize a couple points about this new study below, but you'll need to know a few additional facts as background first...
- There are 80,000 to 100,000 vagus nerve fibers in our bodies. I'll post a study reference link at some point.
- About 80% of these Vagus Nerve Fibers are Sensory (Afferent) and not Motor (Efferent) fibers.
- A good analogy for how this is architected within our bodies: Imagine the broadband network within a city. Large cables carry thousands of smaller wires from the broadband central location out to individual homes. From one point of view, the connection from the central location to the periphery is singular. From another point of view, it's a profound mistake to think about the wire as a single cable. The same is true about the Vagus Nerve and how its presence within us is architected.
Significance
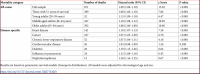
Evolution conferred animals with molecular sensors that monitor cellular and organ function to detect changes in the environment. These activate sensory neural responses that drive the action of reflexes that maintain cellular and physiological homeostasis. Recent advances reveal that neural reflexes modulate the immune system, but it was previously unknown whether cytokine mediators of immunity mediate specific neural signals. Here we develop methods to isolate and decode specific neural signals recorded from the vagus nerve to discriminate between the cytokines IL-1β and TNF. This methodological waveform successfully detects and discriminates between specific cytokine exposures using neural signals.
Abstract
The nervous system maintains physiological homeostasis through reflex pathways that modulate organ function. This process begins when changes in the internal milieu (e.g., blood pressure, temperature, or pH) activate visceral sensory neurons that transmit action potentials along the vagus nerve to the brainstem. IL-1β and TNF, inflammatory cytokines produced by immune cells during infection and injury, and other inflammatory mediators have been implicated in activating sensory action potentials in the vagus nerve. However, it remains unclear whether neural responses encode cytokine-specific information. Here we develop methods to isolate and decode specific neural signals to discriminate between two different cytokines. Nerve impulses recorded from the vagus nerve of mice exposed to IL-1β and TNF were sorted into groups based on their shape and amplitude, and their respective firing rates were computed. This revealed sensory neural groups responding specifically to TNF and IL-1β in a dose-dependent manner. These cytokine-mediated responses were subsequently decoded using a Naive Bayes algorithm that discriminated between no exposure and exposures to IL-1β and TNF (mean successful identification rate 82.9 ± 17.8%, chance level 33%). Recordings obtained in IL-1 receptor-KO mice were devoid of IL-1β–related signals but retained their responses to TNF. Genetic ablation of TRPV1 neurons attenuated the vagus neural signals mediated by IL-1β, and distal lidocaine nerve block attenuated all vagus neural signals recorded. The results obtained in this study using the methodological framework suggest that cytokine-specific information is present in sensory neural signals within the vagus nerve.
Wow!
They put an electrode on an AFFERENT Vagus Nerve fiber and, using Machine Learning techniques, were able to distinguish between two different, key Inflammatory Cytokine Signals, IL-1b and TNF.
Wow!
The details of this study are complicated and I haven't (yet) had time to digest all the details.
In studies of disorders, disease, death, and healthy longevity, we've been seeing, increasingly, how critical Inflammation Expression Inhibition is for healthy longevity.
So, now, understand these two facts together to assess a prediction...
--> Someday, it will be possible to identify and monitor specific Inflammatory Cytokine Expression signals in the Periphery of our bodies to provide an appropriate response...
:-)
Edited by HighDesertWizard, 23 January 2019 - 04:23 PM.