





























Intermittent fasting? Perhaps caloric restriction, but don't body builders use IF to achieve higher levels of IGF1 to grow more muscle?
 LongeCity
LongeCityAdvocacy & Research for Unlimited Lifespans



Posted 29 July 2016 - 10:47 PM
I think it's quite possible to negate some of the harm from smoking, I've seen plenty of trials on Pubmed where they were able to negate some portion of the harm with stuff like green tea, curcumin, mito-targeted antioxidants and so on. If you look for trials looking at what can be done to protect against airborne pollution you can find plenty more.
Totally agree. Just think of the higher need of some antioxidants, for example at least 500mg for smokers, and the damage which already could be prevented through such simple means. Smoking robs the body of C and B-vitamins. Think it's malicious in plain sight of all the science to deny that harm from smoking could not at least be alleviated somewhat. And really stupid not to do for any smoker unwilling or unable to quit.
Micronutrient, metabolic tuning - prevention - therapy, maintaining to quit would be the best prevention, recommends:
1 - 2 g Vitamin C
200 - 1000 IU Vitamin E
5 - 15 mg Carotene Complex
10 - 50 mg Vitamin-B Complex (especially Vitamin B6)
0.4 - 1 mg Folate
50 - 100 mg Vitamin B12
100 - 200 mcg Selen
1000 - 2000 IU Vitamin D3
600 - 1200 mg Calcium (+ Vitamin D, especially female smokers)
200 - 400 mg Magnesium
Don't fully agree with this. Personally got rid of PAD symptoms (intermittent claudication, from 80% stenosis at abdominal aorta) with mega-dosing vitamin C (>18 g/d; Yolf's up-tread warnings about mega-dose vitamin C aren't based on science) and Linus Pauling's therapy. Wouldn't supplement that much alpha-tocopherol without balancing with other mixed tocopherols and tocotrienols. Or supplement Beta-Carotene at all, but Vitamin A, Astaxanthin, Lycopene and Luthein instead. Needed much more Vitamin Bs - especially B6, B9, B12 and TMG - to get Homocysteine down, use methylfolate only and avoid folic acid. Use Vitamin D3 to get my 25(OH)D3 serum levels up to at least 60 ng/dl (in my case 7700 IUs/d), along with vitamin K2. Supplement Calcium and Magnesium in the opposite ratio of 1:2.
Much healing occurred with such comprehensive supplementation started 7 years ago, which all my docs considered impossible but predicted steady worsening instead. Hell, I didn't even get one sunburn since 7 years from all the antioxidants, despite still sun-bathing in tropical sun (without suncream). In my case even the reversal of such a classical smokers disease as PAD has been possible with supplementation and lifestyle changes.
Have been taken most other botanicals and amino-acids already mentioned too:
N-Acetyl-Cysteine, turmeric & pepper. Lots of habanero/cayenne to keep blood flow up. Niacin and B vitamins are crucial. Resveratrol and other antioxidants.
Black tea prevents cigarette smoke-induced apoptosis and lung damage
Green tea protects human osteoblasts from cigarette smoke-induced injury: possible clinical implication
Apple polyphenol protects against cigarette smoke-induced acute lung injury
Carbocisteine protects against emphysema induced by cigarette smoke extract in rats.
Curcumin protects against cigarette smoke-induced cognitive impairment and increased acetylcholinesterase activity in rats
Andrographolide protects against cigarette smoke-induced oxidative lung injury via augmentation of Nrf2 activity.
Beta-carotene protects rats against bronchitis induced by cigarette smoking
Free and nanoencapsulated curcumin prevents cigarette smoke-induced cognitive impairment and redox imbalance.
Curcumin attenuates elastase- and cigarette smoke-induced pulmonary emphysema in mice.
Edited by pamojja, 29 July 2016 - 10:53 PM.
Posted 29 July 2016 - 10:50 PM
N-Acetylcysteine (NAC) and glutathione (GSH): Antioxidant and chemopreventive properties, with special reference to lung cancer
"...The antimutagenic and anticarcinogenic properties of NAC could be ascribed to multiple protective mechanisms, such as NAC nucleophilicity, antioxidant activity, its ability to act as a precursor of intracellular reduced GSH, modulation of detoxification, and DNA repair processes. On these grounds, NAC has emerged as a most promising cancer chemopreventive agent..."
The effects of phenethyl isothiocyanate, N-acetylcysteine and green tea on tobacco smoke-induced lung tumors in strain A/J mice.
Anti-inflammatory and antioxidant effects of resveratrol in healthy smokers a randomized, double-blind, placebo-controlled, cross-over trial.
Inositol May Prevent Lung Cancer in Cigarette Smokers
NAC (N-acetyl-cysteine) reduces the carcinogenicity of tobacco smoke.
Note that Panax Ginseng has an anticancer effect on cancers induced with benzopyrene.
Taurine, "an amino acid present in fish, is able to restore normal blood vessel function in smokers."
Vitamin C prevents cigarette smoke induced atherosclerosis in guinea pig model, Journal of Atherosclerosis and Thrombosis, 2010 Aug 31; 17(8):817-27.
Quercetin...opens up COPD-inflicted airways. It restores normal elasticity of lung tissue and reduces inflammation. Just as important, it reduces production of the protein-melting enzymes that dissolve alveolar walls, helping to retain the lungs' normal architecture and function." - Anne Buckley (2012), Quercetin: Broad-Spectrum Protection, Life Extension Magazine, September 2012. Bharani A, Ahirwar LK, Jain J (2004),
Terminalia arjuna reverses impaired endothelial function in chronic smokers, Indian Heart Journal, 2004 Mar-Apr;56(2):123-8. See Arjuna
Serum B vitamin levels and risk of lung cancer.
CONCLUSION: Serum levels of vitamin B(6) and methionine were inversely associated with risk of lung cancer.
When my smoking habit was at its worst suffered for one year a chronic bronchitis. Therefore limited my daily cigs. to 20 again, started to smoke organically grown tobacco only, stayed for a couple of months at the beach with fresh sea-air and used lots of Ayurvedics to completely clear it up again.
So much is possible. Harm can never be nullified, but reasonably alleviated without pharmaceuticals.
Edited by pamojja, 29 July 2016 - 10:58 PM.

Posted 30 July 2016 - 08:58 PM
I'd like to add that as a former smoker, I find that potent p53 activators and senolytics such as MetaQuercetin, liquid hickory smoke (research first and understand difference between effects of liquid and fat soluble fractions on cancer... don't just take), and resveratrol seem to kill off alot of damaged cells in my lungs and do improve breathing, pheromonal receptivity... the side effects are susceptibility to coughs/pneumonia until the cells get replaced... I take periodic high doses with nitazoxanide (broad spectrum antimicrobial) to prevent.
Also, doesn't B6 lower dopamine, isn't nicotine a dopaminergic? So is B6 really good for quitting? I take P5P periodically, but I can't say I'm fond of the effects of B6... makes me a little lazy, I make my own B Complex.
Pamojja, you sound like you're going to wind up with cancer... I'd really just quit cold turkey.


Posted 31 July 2016 - 12:00 AM
I don't think you understood the context of my phrase. Modern day intellectual-types are much more likely to not smoke because they are now aware of the negative side effects of smoking; hence the oxymoron.
It's well educated people that smoke less, since education is a marker for social programmability.
Since antismoking propaganda (pseudo-science) is optimized for the thick middle section of the IQ Bell Curve where the most of the targets are, the thin low and high tails of the IQ Bell Curve are less susceptible to such indoctrination. At the low end, some of these folks don't care or fully grasp the message, or are natural risk takers, but largely they use it as a poor man's medicine to treat chronic inflammatory & autoimmune diseases (as my earlier post in this thread illustrates in case of rheumatoid arthritis), or to boost their detox rate due to life hardships (smoking doubles catalase and SOD, and increases glutathione by 80%, see the cited thread), or as a potent nootropic (MAOI B, plus additional dopaminergic and cholinergic effects), "the most reliable cognitive enhancer that we currently have". At the high IQ end, they know better, easily seeing through the pseudo-scientific scam.
So you're defending smoking? 

Posted 31 July 2016 - 01:04 PM
Intermittent fasting? Perhaps caloric restriction, but don't body builders use IF to achieve higher levels of IGF1 to grow more muscle?
Bodybuilders use frequent meals of high protein content to achieve maximal IGF-1 levels, coupled with gym of course.
Low meal frequency also lowers IGF-1, especially if you combine it with LCHF-ish diet plans.
Posted 31 July 2016 - 02:14 PM
Bodybuilders use frequent meals of high protein content to achieve maximal IGF-1 levels, coupled with gym of course.
Low meal frequency also lowers IGF-1, especially if you combine it with LCHF-ish diet plans.
Though I don't know what would be considered a low IGF-1. Normal range with my lab is 101 - 267 ng/ml (optimal I read somewhere 90 - 249) - mine has been declining from 194 in 2011 to 161 last year, now at 139 ng/nl. On 2 LCHF-ish meals a day, with a 15 hrs fasting window and skipping meals completely at times.
Edited by pamojja, 31 July 2016 - 02:18 PM.
Posted 31 July 2016 - 04:25 PM
Pamojja, you sound like you're going to wind up with cancer... I'd really just quit cold turkey.
How would anyone know, other than someone with a God-complex or brainwashed?
Just read on a packet:
Smoking will increase your risk of dying, why not quit now?
With the same kind of naive reasoning wouldn't one have to come to the logical conclusion?
Living has a 100% change of dying, why not quit now?
I always abhorred such simplistic reasoning, since I saw how such negative believes would move smokers - willing, but yet unable to quit - in a down-ward spiral, further weakening their self-confidence needed for quiting. And unknowingly taken for a ride on the Noceebo effect.
To counter that, it helps to be more realistic, even if all we have is epidemiological data. Statistically my gender, age and origin I have a live expectancy 66.5 years (http://www.worldlife...life-expectancy), that's 17 years from now.
Seems already very unlikely and at odds, considering my medical history:
Pneumonia at birth (already predestined for COPD, additional tetracyclines given against ruined all my teeth), fever fits at 2, lots of antibiotics against recurring infections during early childhood, meningitis with 7, sometime before 20 tuberculosis, malaria: 4 x tropica, 3x vivax, amoebic hepatitis with NAFDL, and a spinal cord infection between age 27-32, after onset of rhinitis and schistosomiasis with 39, PAD with only 3-400m pain-free walking distance at age 41 (and predicted a 30% change of dying in the next 5 years despite pharmaceutical and operative intervention, which I refused).
Came a long way in surviving things which could have easily been deathly already. Looking at my genes, both grandmothers diet around their 80iest year (non-smokers). Both grandfathers died much earlier (smokers): one exactly my age from tuberculosis, the other - with bouts of serious depression - dropped death while praying in church the year I was born. No cancers in my family.
Very likely because both smoking grandfathers didn't reach the age lung cancer usually manifest, with its highest rate at age 80 (compare that to my already unrealistic live expectancy of 66.5 years):
http://www.ncbi.nlm....les/PMC3399915/
 nihms388387f1.jpg 36.6KB
1 downloads
nihms388387f1.jpg 36.6KB
1 downloads
Age-specific death rates (per 100,000) in the Unites States in 1950 and 2004
http://jnci.oxfordjo...t/95/6/470.long
 Clipboard01.png 26.97KB
1 downloads
Clipboard01.png 26.97KB
1 downloads
Approximate 10-year risk of developing lung cancer
Therefore speculating with the unlikelihood of still smoking at the peak of my live-expectancy at 66.5 years of age, at that time I would have a 11% risk of dying within 10 years from lung cancer, 8% if I quit at that time. Quiting earlier the chances of dying from lung cancer the next 10 years would proportionally decrease from 7% to 4%.
Pamojja, you sound like you're going to wind up with cancer... I'd really just quit cold turkey.
However, I still encourage everyone to quit smoking based on these statistical facts, not the usual completely unreasonable fear-mongering and ostracism against smokers.
War against cancer, war against drugs, war against terrorists, and war against smokers. We know where all these wars lead: profits for a few.

Posted 31 July 2016 - 11:35 PM
Pamojja, you sound like you're going to wind up with cancer... I'd really just quit cold turkey.
How would anyone know, other than someone with a God-complex or brainwashed?
Just read on a packet:
Smoking will increase your risk of dying, why not quit now?
With the same kind of naive reasoning wouldn't one have to come to the logical conclusion?
Living has a 100% change of dying, why not quit now?
I always abhorred such simplistic reasoning, since I saw how such negative believes would move smokers - willing, but yet unable to quit - in a down-ward spiral, further weakening their self-confidence needed for quiting. And unknowingly taken for a ride on the Noceebo effect.
To counter that, it helps to be more realistic, even if all we have is epidemiological data. Statistically my gender, age and origin I have a live expectancy 66.5 years (http://www.worldlife...life-expectancy), that's 17 years from now.
Seems already very unlikely and at odds, considering my medical history:
Pneumonia at birth (already predestined for COPD, additional tetracyclines given against ruined all my teeth), fever fits at 2, lots of antibiotics against recurring infections during early childhood, meningitis with 7, sometime before 20 tuberculosis, malaria: 4 x tropica, 3x vivax, amoebic hepatitis with NAFDL, and a spinal cord infection between age 27-32, after onset of rhinitis and schistosomiasis with 39, PAD with only 3-400m pain-free walking distance at age 41 (and predicted a 30% change of dying in the next 5 years despite pharmaceutical and operative intervention, which I refused).
Came a long way in surviving things which could have easily been deathly already. Looking at my genes, both grandmothers diet around their 80iest year (non-smokers). Both grandfathers died much earlier (smokers): one exactly my age from tuberculosis, the other - with bouts of serious depression - dropped death while praying in church the year I was born. No cancers in my family.
Very likely because both smoking grandfathers didn't reach the age lung cancer usually manifest, with its highest rate at age 80 (compare that to my already unrealistic live expectancy of 66.5 years):
http://www.ncbi.nlm....les/PMC3399915/
Age-specific death rates (per 100,000) in the Unites States in 1950 and 2004
http://jnci.oxfordjo...t/95/6/470.long
Approximate 10-year risk of developing lung cancer
Therefore speculating with the unlikelihood of still smoking at the peak of my live-expectancy at 66.5 years of age, at that time I would have a 11% risk of dying within 10 years from lung cancer, 8% if I quit at that time. Quiting earlier the chances of dying from lung cancer the next 10 years would proportionally decrease from 7% to 4%.
For a mere 3% to 6% risk reduction (from 10 to 25 years) in lung cancer? ..you must be joking!I rather sound like to wind up with a 89% chance of dying of anything else than lung cancer at my peak live expectancy of 66.5 years.
However, I still encourage everyone to quit smoking based on these statistical facts, not the usual completely unreasonable fear-mongering and ostracism against smokers.
War against cancer, war against drugs, war against terrorists, and war against smokers. We know where all these wars lead: profits for a few.
Smoking has a widely distributed negative effect upon the whole body, it affects many physiological system and is involved in pathogenesis of many, many diseases! But putting this aside, war against smokers do not profit 'few'.
In the UK, for example, taxation from cigarette imports is massive, cigarette companies are massive. However, strain is felt by the people whom have to pay for the healthcare of smokers due to the socialist health care system in the UK. Who are these 'few' it profits apart from the public?
Posted 01 August 2016 - 10:08 AM
However, I still encourage everyone to quit smoking based on these statistical facts, not the usual completely unreasonable fear-mongering and ostracism against smokers.
War against cancer, war against drugs, war against terrorists, and war against smokers. We know where all these wars lead: profits for a few.
Smoking has a widely distributed negative effect upon the whole body, it affects many physiological system and is involved in pathogenesis of many, many diseases! But putting this aside, war against smokers do not profit 'few'.
In the UK, for example, taxation from cigarette imports is massive, cigarette companies are massive. However, strain is felt by the people whom have to pay for the healthcare of smokers due to the socialist health care system in the UK. Who are these 'few' it profits apart from the public?
Sure is only that a smoker typically dies either of a smoking related or non-related disease, chances are about fifty/fifty. Don't know the exact distribution of diseases in non-smokers, but in total it makes 100% too.
Gave some analogies for potentially 'few'. You could also follow the money, the monopolization and power. Or you directly take the Orwellian "war is peace, freedom is slavery, ignorance is strength" as a hind..
But I beg you to reconsider your stance about our 'socialist' health care system (rather a sickness industry anyway). All 4 of my grandparents were hard-working people. Would you really despise my 2 non-smoking grandmothers, because only they received a quarter-century worth of monthly pensions, and multiple prescriptions-medication their last decade? But my smoking and suddenly dying grandfathers not a penny, Sith?

Posted 01 August 2016 - 03:11 PM
All 4 of my grandparents were hard-working people. Would you really despise my 2 non-smoking grandmothers, because only they received a quarter-century worth of monthly pensions, and multiple prescriptions-medication their last decade? But my smoking and suddenly dying grandfathers not a penny, Sith
Add to that both my non-smoking parents, and you end up now with a whole century worth of monthly pension payments, hip-replacements, prostrate surgery and radiation, multiple medications, regular examinations and physiotherapies, exclusively on a account of my non-smoking ancestors.
Lifetime Medical Costs of Obesity: Prevention No Cure for Increasing Health Expenditure
Background
Obesity is a major cause of morbidity and mortality and is associated with high medical expenditures. It has been suggested that obesity prevention could result in cost savings. The objective of this study was to estimate the annual and lifetime medical costs attributable to obesity, to compare those to similar costs attributable to smoking, and to discuss the implications for prevention.
Methods and Findings
With a simulation model, lifetime health-care costs were estimated for a cohort of obese people aged 20 y at baseline. To assess the impact of obesity, comparisons were made with similar cohorts of smokers and “healthy-living” persons (defined as nonsmokers with a body mass index between 18.5 and 25). Except for relative risk values, all input parameters of the simulation model were based on data from The Netherlands. In sensitivity analyses the effects of epidemiologic parameters and cost definitions were assessed. Until age 56 y, annual health expenditure was highest for obese people. At older ages, smokers incurred higher costs. Because of differences in life expectancy, however, lifetime health expenditure was highest among healthy-living people and lowest for smokers. Obese individuals held an intermediate position. Alternative values of epidemiologic parameters and cost definitions did not alter these conclusions.
Conclusions
Although effective obesity prevention leads to a decrease in costs of obesity-related diseases, this decrease is offset by cost increases due to diseases unrelated to obesity in life-years gained. Obesity prevention may be an important and cost-effective way of improving public health, but it is not a cure for increasing health expenditures.
The lifetime costs were in Euros:
Healthy: 281,000
Obese: 250,000
Smokers: 220,000
journal.pmed.0050029.t001.png 246.43KB
0 downloads
Edited by pamojja, 01 August 2016 - 04:06 PM.
Posted 03 August 2016 - 11:59 AM
Use of Glucosamine and Chondroitin and Lung Cancer Risk in the VITamins And Lifestyle (VITAL) Cohort
Results
High 10-year use of glucosamine [Hazard Ratio (HR) 0.77, 95% CI: 0.56–1.07; P-trend=0.04] but not chondroitin was associated with a reduction in lung cancer risk. The association with glucosamine was limited to adenocarcinoma (HR 0.49, 95% CI: 0.27–0.90; Ptrend-<0.01), and was not modified by NSAID use or smoking status.
Posted 04 August 2016 - 05:41 PM
How would anyone know, other than someone with a God-complex or brainwashed?
Just read on a packet:
Smoking will increase your risk of dying, why not quit now?
With the same kind of naive reasoning wouldn't one have to come to the logical conclusion?
Living has a 100% change of dying, why not quit now?
I always abhorred such simplistic reasoning, since I saw how such negative believes would move smokers - willing, but yet unable to quit - in a down-ward spiral, further weakening their self-confidence needed for quiting. And unknowingly taken for a ride on the Noceebo effect.
To counter that, it helps to be more realistic, even if all we have is epidemiological data. Statistically my gender, age and origin I have a live expectancy 66.5 years (http://www.worldlife...life-expectancy), that's 17 years from now.
Seems already very unlikely and at odds, considering my medical history:
Pneumonia at birth (already predestined for COPD, additional tetracyclines given against ruined all my teeth), fever fits at 2, lots of antibiotics against recurring infections during early childhood, meningitis with 7, sometime before 20 tuberculosis, malaria: 4 x tropica, 3x vivax, amoebic hepatitis with NAFDL, and a spinal cord infection between age 27-32, after onset of rhinitis and schistosomiasis with 39, PAD with only 3-400m pain-free walking distance at age 41 (and predicted a 30% change of dying in the next 5 years despite pharmaceutical and operative intervention, which I refused).
Came a long way in surviving things which could have easily been deathly already. Looking at my genes, both grandmothers diet around their 80iest year (non-smokers). Both grandfathers died much earlier (smokers): one exactly my age from tuberculosis, the other - with bouts of serious depression - dropped death while praying in church the year I was born. No cancers in my family.
Very likely because both smoking grandfathers didn't reach the age lung cancer usually manifest, with its highest rate at age 80 (compare that to my already unrealistic live expectancy of 66.5 years):
http://www.ncbi.nlm....les/PMC3399915/
Age-specific death rates (per 100,000) in the Unites States in 1950 and 2004
http://jnci.oxfordjo...t/95/6/470.long
Approximate 10-year risk of developing lung cancer
Therefore speculating with the unlikelihood of still smoking at the peak of my live-expectancy at 66.5 years of age, at that time I would have a 11% risk of dying within 10 years from lung cancer, 8% if I quit at that time. Quiting earlier the chances of dying from lung cancer the next 10 years would proportionally decrease from 7% to 4%.
Pamojja, you sound like you're going to wind up with cancer... I'd really just quit cold turkey.For a mere 3% to 6% risk reduction (from 10 to 25 years) in lung cancer? ..you must be joking!I rather sound like to wind up with a 89% chance of dying of anything else than lung cancer at my peak live expectancy of 66.5 years.
However, I still encourage everyone to quit smoking based on these statistical facts, not the usual completely unreasonable fear-mongering and ostracism against smokers.
War against cancer, war against drugs, war against terrorists, and war against smokers. We know where all these wars lead: profits for a few.
Silly reasoning, not going to read it all, but why accumulate smoking byproducts if you don't have to? Sure a tiny fraction of a percent will live longer for smoking, but assuming our mission succeeds, they wouldn't get much further...

Posted 06 August 2016 - 11:53 AM
Pamojja, you sound like you're going to wind up with cancer... I'd really just quit cold turkey.
Silly reasoning, not going to read it all, but why accumulate smoking byproducts if you don't have to? Sure a tiny fraction of a percent will live longer for smoking, but assuming our mission succeeds, they wouldn't get much further...
You didn't read it, but made already up your mind? How prejudiced. I didn't even argued that..
α-Tocopherol disappearance is faster in cigarette smokers and is inversely related to their ascorbic acid status
Ascorbate attenuates pulmonary emphysema by inhibiting tobacco smoke and Rtp801-triggered lung protein modification and proteolysis
Posted 08 August 2016 - 12:59 AM
However, I still encourage everyone to quit smoking based on these statistical facts, not the usual completely unreasonable fear-mongering and ostracism against smokers.
War against cancer, war against drugs, war against terrorists, and war against smokers. We know where all these wars lead: profits for a few.
Smoking has a widely distributed negative effect upon the whole body, it affects many physiological system and is involved in pathogenesis of many, many diseases! But putting this aside, war against smokers do not profit 'few'.
In the UK, for example, taxation from cigarette imports is massive, cigarette companies are massive. However, strain is felt by the people whom have to pay for the healthcare of smokers due to the socialist health care system in the UK. Who are these 'few' it profits apart from the public?
Sure is only that a smoker typically dies either of a smoking related or non-related disease, chances are about fifty/fifty. Don't know the exact distribution of diseases in non-smokers, but in total it makes 100% too.
Gave some analogies for potentially 'few'. You could also follow the money, the monopolization and power. Or you directly take the Orwellian "war is peace, freedom is slavery, ignorance is strength" as a hind..
But I beg you to reconsider your stance about our 'socialist' health care system (rather a sickness industry anyway). All 4 of my grandparents were hard-working people. Would you really despise my 2 non-smoking grandmothers, because only they received a quarter-century worth of monthly pensions, and multiple prescriptions-medication their last decade? But my smoking and suddenly dying grandfathers not a penny, Sith?
I respect your passion for Smoking but you're only fooling yourself here... Sorry to say.
Posted 08 August 2016 - 09:20 AM
I respect your passion for Smoking but you're only fooling yourself here... Sorry to say.
I don't have passion for or against smoking. But against endless unscientific accusations because of unfounded prejudices. You're the one fooling yourself.
It's well educated people that smoke less, since education is a marker for social programmability.
Since antismoking propaganda (pseudo-science) is optimized for the thick middle section of the IQ Bell Curve where the most of the targets are, the thin low and high tails of the IQ Bell Curve are less susceptible to such indoctrination. At the low end, some of these folks don't care or fully grasp the message, or are natural risk takers, but largely they use it as a poor man's medicine to treat chronic inflammatory & autoimmune diseases (as my earlier post in this thread illustrates in case of rheumatoid arthritis), or to boost their detox rate due to life hardships (smoking doubles catalase and SOD, and increases glutathione by 80%, see the cited thread), or as a potent nootropic (MAOI B, plus additional dopaminergic and cholinergic effects), "the most reliable cognitive enhancer that we currently have". At the high IQ end, they know better, easily seeing through the pseudo-scientific scam.
So you're defending smoking?
If you attack with unfounded prejudices, you have to reckon with counter arguments.
Edited by pamojja, 08 August 2016 - 09:54 AM.


Posted 08 August 2016 - 09:54 AM
I don't have passion for or against smoking. But against endless unscientific accusations because of unfounded prejudices. You're the one fooling yourself.
What about other cancers that smoking increases, and more importantly, the risk of heart disease? Would you quit if you had a heart-attack?
Edited by platypus, 08 August 2016 - 09:54 AM.
Posted 08 August 2016 - 11:05 AM
I don't have passion for or against smoking. But against endless unscientific accusations because of unfounded prejudices. You're the one fooling yourself.
What about other cancers that smoking increases, and more importantly, the risk of heart disease? Would you quit if you had a heart-attack?
Depends on the circumstances. When I was diagnosed a 80% stenosis at the abdominal aorta - with a 30% chance of dying from this condition within 5 years and a mere 3-400 pain-free walking distance - at first I followed the medical advise to quit smoking and doing regular walking exercises. Since it became worse, despite following these recommended interventions, I dug a bid deeper about this classical 'smokers leg'... Well, the changes of quit smoking to prevent this with age always advancing disease are 5.5%. Once one already got it full blown, like me, quiting doesn't make the prospects anything less bleak..
Risk Factor Profile of Nonsmokers with Peripheral Arterial Disease: "In the 561 subjects who had never smoked, 32 (5.7%) had PAD as compared with 12.3% in ex-smokers and 17.8% in current smokers."
After a couple of months exclusively deteriorating I reconsidered, quit these useless interventions, quit anything with sugar, and started Linus Pauling's recommendations for CVD (except the one about quiting to smoke, which already had showed insufficient to turn it around). Only once I reached the therapeutic threshold of his nutrient recommendations my condition improved. After 1 year could walk 1 hour without pain again, 2 hrs the second year, going moderately low carb/high fat. Since spring last year the debilitating symptoms of intermittent claudication are for the first time completely gone, despite having been governmentally certified a 60% disability due to this PAD (which usually isn't reversible). Only CFS-symptoms remaining, but still improving. Have even been able to sustain myself through work I love.
So it depends on experimental trials, and the prospects of turning the wheel around with specific interventions. Which I already have been able to do with a number of deathly diseases, mostly by refusing expensive interventions by 'professionals', after ascertaining their benefits/risks profile. The statistical chances of dying from cancer or CVD look that tiny when one already has suffered, survived and recovered from real potentially deathly diseases, like: PAD, Discitis, Schistosomiasis, Malaria tropica, Tb, Psoriasis, Meningitis, Pneumonia at birth..
Therefore speculating with the unlikelihood of still smoking at the peak of my live-expectancy at 66.5 years of age, at that time I would have a 11% risk of dying within 10 years from lung cancer, 8% if I quit at that time. Quiting earlier the chances of dying from lung cancer the next 10 years would proportionally decrease from 7% to 4%
Posted 08 August 2016 - 11:14 AM
So it depends on experimental trials, and the prospects of turning the wheel around with specific interventions. Which I already have been able to do with a number of deathly diseases, mostly by refusing expensive interventions by 'professionals', after ascertaining their benefits/risks profile. The statistical chances of dying from cancer or CVD look that tiny when one already has suffered, survived and recovered from real potentially deathly diseases, like: PAD, Discitis, Schistosomiasis, Malaria tropica, Tb, Psoriasis, Meningitis, Pneumonia at birth..
Don't succumb to magical thinking - surviving dangerous conditions in the past does not increase your odds of beating smoking-related diseases.
Posted 08 August 2016 - 11:48 AM
Don't succumb to magical thinking - surviving dangerous conditions in the past does not increase your odds of beating smoking-related diseases.
And the odds of other also age-related diseases. 
Sure is only that a smoker typically dies either of a smoking related or non-related disease, chances are about fifty/fifty. Don't know the exact distribution of diseases in non-smokers, but in total it makes 100% too.
Posted 08 August 2016 - 12:09 PM
Cannot you cut down on the number of daily cigarettes smoked and switch partly to vaping? I've seen many longtime smokers to make this switch so it's certainly doable.
Did that already to clear up a persistent bronchitis.
When my smoking habit was at its worst suffered for one year a chronic bronchitis. Therefore limited my daily cigs. to 20 again, started to smoke organically grown tobacco only, stayed for a couple of months at the beach with fresh sea-air and used lots of Ayurvedics to completely clear it up again.
Also whenever on mediation retreats I don't smoke. In all the times when I didn't smoke at all couldn't mention any improvement in my physical well-being - contrary to the many testimonies of former-smoker here.
Personally wouldn't change, since the benefits/risk ratio of smoking tobacco is pretty well known, which can't be said about vaping at this point. My primary doc would instantly prescribe me a SRRI for quiting. Here again, I consider their benefits/risk ratio also in favor of smoking:
http://www.madinamer...antsdepression/
Edited by pamojja, 08 August 2016 - 12:17 PM.
Posted 08 August 2016 - 09:07 PM
10 cigs a day with unlimited vaping would be most probably clearly less unhealthy than smoking a pack a day.
Look at this chart again:
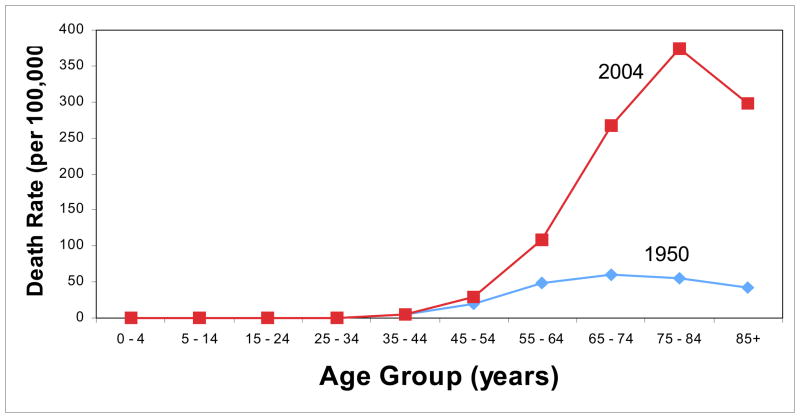
Most start smoking in their teens, and highest occurrence of lung cancer is in the 80ties. So it takes about 60 years for lung cancer to develop. How long are vapers on the market?
Science most probable clearly says: it doesn't know yet.
I do take risks/benefits, but not with something that unknowable. To put it everything into perspective, again:
Worldwide
It is estimated that of the roughly 150,000 people who die each day across the globe, about two thirds—100,000 per day—die of age-related causes because they have aged.[2] In industrialized nations the proportion is much higher, reaching 90%.[2] Thus, albeit indirectly, biological aging (senescence) is by far the leading cause of death. Whether senescence as a biological process itself can be slowed down, halted, or even reversed is a subject of current scientific speculation and research.[3]
So in industrialized nations actually 90% die of age-related causes. That leaves only 10% for the remaining preventable causes (relevant to industrialized nations): Hypertension, Smoking, Medical errors, Poor diet, Overweight, Physical inactivity and Alcohol. Of which I've got only one, and am personally ready to take it's risks.
How about you?
Edited by pamojja, 08 August 2016 - 09:36 PM.
Posted 08 August 2016 - 10:31 PM
The number of chemicals in flavorless vaping solution is so small that it should be easy to assess their carcinogenic and atherogenic potential, so it will not be necessary to wait 100 years to make conclusions. The same cannot be said about tobacco smoke which has circa 4000 chemicals in it according to some sources.
Posted 09 August 2016 - 11:01 PM
... roughly 150,000 people who die each day across the globe, about two thirds—100,000 per day—die of age-related causes because they have aged.[2] In industrialized nations the proportion is much higher, reaching 90%.[2]
Turns out the Wikipedia reference is only secondary and actually an article by Aubrey de Grey:
Aging kills roughly 100,000 people every day worldwide.1 Things that kill far fewer than 1% of this number are the subject of concerted efforts on the part of society to combat them and save these lives, yet aging is studied mainly as a phenomenon to be understood, rather in the way that astronomers study galaxies; doing anything about it is not generally prioritised. Why?
Posted 12 August 2016 - 01:36 PM
Avoidance of sun exposure as a risk factor for major causes of death
RESULTS: ... Nonsmokers who avoided sun exposure had a life expectancy similar to smokers in the highest sun exposure group, indicating that avoidance of sun exposure is a risk factor for death of a similar magnitude as smoking. Compared to the highest sun exposure group, life expectancy of avoiders of sun exposure was reduced by 0.6-2.1 years.
Some abstracts from GreenMedInfo concerning smoking cessation:
Acupuncture treatment ameliorated the smoking withdrawal symptoms as well as the selective attention to smoking-related visual cues in smokers.Pubmed Data : Neurol Res. 2010 Feb;32 Suppl 1:27-30. PMID: 20034441Essential oils of black pepper and angelica reduced the level of nicotine craving and allowed a longer delay before next use of tobacco.Jul 31, 2013Pubmed Data : J Altern Complement Med. 2013 Aug ;19(8):709-13. Epub 2013 Mar 28. PMID: 23536963Exercise interventions may be used as nicotine replacement therapy or protective aids against smoking-related cardiopulmonary disorders.Pubmed Data : J Phys Ther Sci. 2016 Mar ;28(3):983-91. Epub 2016 Mar 31. PMID: 27134398Five minutes of moderate intensity exercise is associated with a short-term reduction in desire to smoke and tobacco withdrawal symptoms.Pubmed Data : Psychopharmacology (Berl). 2004 Jul;174(3):320-6. Epub 2004 Mar 2. PMID: 14997270Fresh lime appears to help those who are attempting to stop smoking.Pubmed Data : J Med Assoc Thai. 2012 Dec ;95 Suppl 12:S76-82. PMID: 23513469Hypnosis combined with nicotine patches compares favorably to standard behavioral counseling for smoking cessation.Pubmed Data : Nicotine Tob Res. 2008 May;10(5):811-8. PMID: 18569754In a meta-analysis of 59 studies hypnosis was judged to be partially efficacious in the treatment of smoking cessation.Pubmed Data : Int J Clin Exp Hypn. 2000 Apr;48(2):195-224. PMID: 10769984Inhalation of vapor from black pepper reduces smoking withdrawal symptoms.Pubmed Data : Drug Alcohol Depend. 1994 Feb;34(3):225-9. PMID: 8033760Intensive behavioral treatment is suprior to brief counseling plus information pamphlet and self-help program with telephone follow-up for smoking cessation.Pubmed Data : J Pharm Pharmacol. 2006 Dec;58(12):1677-82. PMID: 20099536Intensive hypnotherapy for smoking cessation was shown to have a 40% success rate at 26 weeks.Pubmed Data : Int J Clin Exp Hypn. 2006 Jul;54(3):303-15. PMID: 16766441Mindfulness-based interventions reduce the urge to smoke in college student smokers.Pubmed Data : Psychol Addict Behav. 2009 Dec;23(4):666-71. PMID: 20025372Physical activity appears to be an effective strategy for maintaining tobacco abstinence.Pubmed Data : Prev Med. 2008 Aug;47(2):215-20. Epub 2008 May 16. PMID: 18572233Smoking cravings are reduced by self-massage.Pubmed Data : Prev Med. 1999 Jan;28(1):28-32. PMID: 9973585Benfotiamine, a form of thiamine, attenuates nicotine and uric acid-induced vascular endothelial dysfunction in the rat.Pubmed Data : Pharmacol Res. 2008 Nov-Dec;58(5-6):356-63. Epub 2008 Oct 2. PMID: 18951979Coptidis Rhizoma attenuates repeated nicotine-induced behavioural sensitization in the rat.Pubmed Data : J Pharm Pharmacol. 2007 Dec;59(12):1663-9. PMID: 18053328Rhodiola rosea has a therapeutic effect in the treatment of smoking cessation.Pubmed Data : Swed Dent J. 2006;30(2):55-60. PMID: 19939867St. Johns Wort attenuates nicotine withdrawal signs in mice.Pubmed Data : Psychopharmacology (Berl). 2003 Sep;169(2):186-9. Epub 2003 Apr 29. PMID: 12719964St. Johns Wort may be therapeutic in the treatment of nicotine addiction.Pubmed Data : Phytother Res. 2009 Jul 7. PMID: 19585471Males are more likely to report smoking abstinence than female participants following hypnosis-based treatments for smoking.Pubmed Data :Int J Clin Exp Hypn. 2006 Apr;54(2):224-33. PMID: 16581692
Edited by pamojja, 12 August 2016 - 01:48 PM.
Posted 13 August 2016 - 12:09 PM
Benfotiamine, a form of thiamine, attenuates nicotine and uric acid-induced vascular endothelial dysfunction in the rat.Pubmed Data : Pharmacol Res. 2008 Nov-Dec;58(5-6):356-63. Epub 2008 Oct 2. PMID: 18951979Coptidis Rhizoma (Berberine) attenuates repeated nicotine-induced behavioural sensitization in the rat.Pubmed Data : J Pharm Pharmacol. 2007 Dec;59(12):1663-9. PMID: 18053328
2 further from the same side
10-day broccoli consumption has a significant effect on the inflammatory status of young healthy smokersPubmed Data : Int J Food Sci Nutr. 2014 Feb ;65(1):106-11. Epub 2013 Sep 2. PMID: 23992556Hydroxocobalamin has a therapeutic effect in acute cyanide poisoning in smoke inhalationPubmed Data : Ann Emerg Med. 2007 Jun;49(6):794-801, 801.e1-2. Epub 2007 May 4. PMID: 17481777
Posted 22 January 2017 - 11:47 AM
I think the intelligent smoker should switch to natural tobacco, preferably in a pipe. Even if one doesn't buy Nightlight's (who is a genius in my opinion) arguments, Surgeon General's landmark report on smoking (1964) showed that pipe smokers live longer than non-smokers. As anti-smoking hysteria intensified, later reports have glossed over this fact and nowadays 'we know' that even a whiff of second-hand smoke (in a park) will kill you. 










Science & Health →
AgingResearch →
Lipid Soluble Alkaloids: Theobromine / Caffeine / Nicotine / QuinineStarted by Dorian Grey , 01 Aug 2025 |
|

|
||
Science & Health →
Lifestyle →
Sleep hacks for counteracting Nicotine's negative effect on sleep?Started by jroseland , 21 Dec 2024 |
|

|
||
Science & Health →
Supplements →
Nicotine as a SupplementStarted by sub7 , 16 Feb 2024 |
|
|
||
Science & Health →
Brain Health →
Nootropic Stacks →
Best RoA for NicotineStarted by Valvolt , 11 Feb 2022 |
|

|
||
Science & Health →
Supplements →
Best supplements for healing the lungsStarted by MikeGreo , 08 Aug 2021 |
|

|
0 members, 1 guests, 0 anonymous users


Community Forum Software by IP.Board
Licensed to: ImmInst.org




