Much of this has been mentioned before, but i am fairly interested in the gotu kola + pycnogenol combination. Life extension has a decent write up on it, and a nice trickle of studies keep coming in.
It increases macro and microvascular blood flow, which is nice.
https://www.lifeexte...arterial-plaque
https://pubmed.ncbi....h.gov/31633315/
"Considering a 34.88% increase in SM subjects, the total absolute difference between SM (34.8%) and the decrease observed in group 3 (-9.95%) was 44.75% (P<0.02)."
https://pubmed.ncbi....h.gov/31625707/ (with aspirin as well)
"In comparison with the SM group and the cardioaspirin group the rate of 'hard' cardiovascular events, requiring hospital admissions were <4% with the combined supplement in comparison with a value >12% in the other two groups (22.22% event rate in the SM group)."
I believe that the glycocalx in important the prevention on damage, it deteriorates with age and can be protected by reducing inflammation, hyperglycemia etc. Exercise helps improve it as well.
https://sjtrem.biome...3049-016-0239-y
INTERESTINGLY though, there is some research showing that it can be repaired/supported by two of our handy little friends already mentioned earlier in, glucosamine and chondroitin.
Glucosamine is a precurser for gags that are involved in the glycocalx, which could potentially come in handy if synthesis slows down in old age OR damage outpaces repair. I dont know how much it contributes though.
chondroitin happens to be an important part of the glycocalx and is associated with reduced risk of heart attack.
Although its possible the effect is only in the unhealthy or old.
"The reduced risk among current users was observed in both short-term (<365 days, AOR = 0.58; 95%CI: 0.45–0.75) and long-term users (>364 days AOR = 0.56; 95%CI:0.36–0.87),
in both sexes (men, AOR = 0.52; 95%CI:0.38–0.70; women, AOR = 0.65; 95%CI:0.46–0.91), in individuals over or under 70 years of age (AOR = 0.54; 95%CI:0.38–0.77,
and AOR = 0.61; 95%CI:0.45–0.82, respectively) and in individuals at intermediate (AOR = 0.65; 95%CI:0.48–0.91) and high cardiovascular risk (AOR = 0.48; 95%CI:0.27–0.83),
but not in those at low risk (AOR = 1.11; 95%CI:0.48–2.56)."
I suspect that gags are high in commercially available gelatin but i have no clue how much would be in there.
https://pubmed.ncbi....h.gov/16308135/ this study at the very least shows gag increase in bone after shark collagen administration to rats, so thats something.
As for getting the plaque out, i'm looking at fasting as a potential way to do that.
First of all. in mice "IF can reduce circulating pro-inflammatory monocytes and adhesion of these cells to endothelium, another anti-atherogenic mechanisms of IF treatment."
"IF potentially increases plaque stability by increasing collagen and VSMC content, while decreasing necrotic cores and macrophage/foam cell content."
https://faseb.online...pplement.786.30
Prolonged fasting increases the cholesterol efflux capacity and anti-inflammatory functionality of HDL particles in human subjects.
"we found that PF induces stark improvements in the functionality of HDL particles. PF increases the ability of HDL to promote cholesterol efflux from cholesterol-loaded THP-1 monocytes and increases the ability of HDL to suppress TNF-α secretion from primary macrophage stimulated with pro-inflammatory citrullinated-fibrinogen immune complexes. Furthermore, increased fasting duration was directly associated with increased Reverse cholesterol transport (RCT) ability and increased anti-inflammatory capacity of HDL with the maximal effect being reached after 36hrs of fasting. To our knowledge, this is the first study to show that PF is capable of improving the RCT ability of HDL and modifying the immunomodulatory functionality of HDL towards a more anti-inflammatory phenotype. These results thereby suggest that HDL may represent a novel mechanism by which PF exerts a portion of its systemic anti-inflammatory and cardioprotective effects."
As for inflammation this caught my eye (curcumin is also in my stack): https://pubmed.ncbi....h.gov/35033882/
The omega-3 index is inversely associated with the neutrophil-lymphocyte ratio in adults'
"The neutrophil-lymphocyte ratio (NLR) is a biomarker of systemic inflammation and measures innate-adaptive immune system balance. The omega-3-index (O3I) measures the amount of EPA+DHA in blood. Both a low O3I and an elevated NLR are associated with increased risk for chronic disease and mortality, including cardiovascular diseases and cancer. Hypothesizing that low O3I may partly contribute to systemic chronic inflammation, we asked if a relationship existed between O3I and NLR in healthy adults (≥18 y, n = 28,871, 51% female) without inflammation [C-reactive protein (CRP) <3 mg/mL)] who underwent a routine clinical assessment. NLR was inversely associated with O3I before (p < 0.0001) and after adjusting for age, sex, BMI, and CRP (p < 0.0001). Pearson correlations of other variables with NLR were r = 0.06 (CRP), r = 0.14 (age), and r = 0.01(BMI). In this healthy population, an O3I < 6.6% was associated with increasing NLR whereas NLR remained relatively constant (low) when O3I > 6.6%, suggestive of a quiescent, balanced immune system."
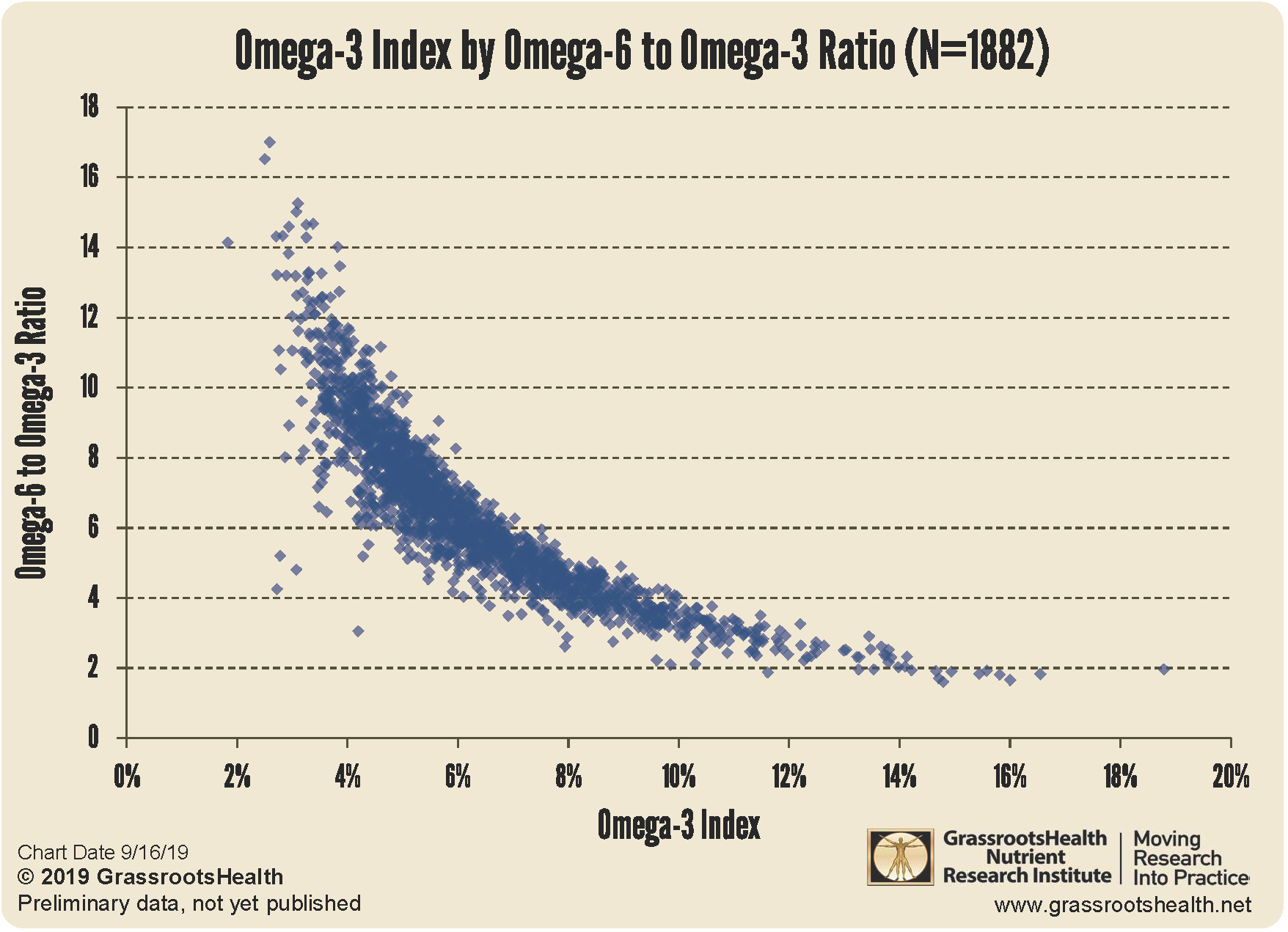
Whats more is omega 3/6 ratio looks like it may matter quite a bit in this regard, looking on grassroots health. It took a ratio of 1:4 to get everyone over the 6% omega index line.
https://www.grassroo...-aa-epa-ratios/
Generally, i think preventing damage as much as possible with lifestyle. Taking a few select supplements (the above for example, k2+mag+d etc) and doing a fast every once in a while is a fairly good approach.


































 LongeCity
LongeCity




























