warner, On this topic of glaucoma and NR I think there is enough interest to dedicate a entire thread to this. Without question the neuroprotective effects seem to be what suffers of glaucoma would benefit from. I would also begin to research "nicotinamide riboside mitochondrial biogenesis" because increasing mitochondrial numbers within the cells of the eye would likely be of benefit. These effects have been associated with NR along with the SIRT1 and SIRT3 increases. I would also look over the previous post on the NLRP3 Inflammasome. All together Increasing cellular respiration, decreasing low-grade inflammation, increasing mitochondrial numbers and boosting NAD reserves seems to be a desired set of conditions in ameliorating many disease states not just glaucoma.
Hey bluemoon, I guess I'm the keeper of the data and can find most of what your asking. What I hope to learn is how long a single dose of NR carries us thru the day. I've contacted 2 researchers and ChromaDex directly chasing this answer. I've been asked to wait as the data is correlated and the longterm study is completed.
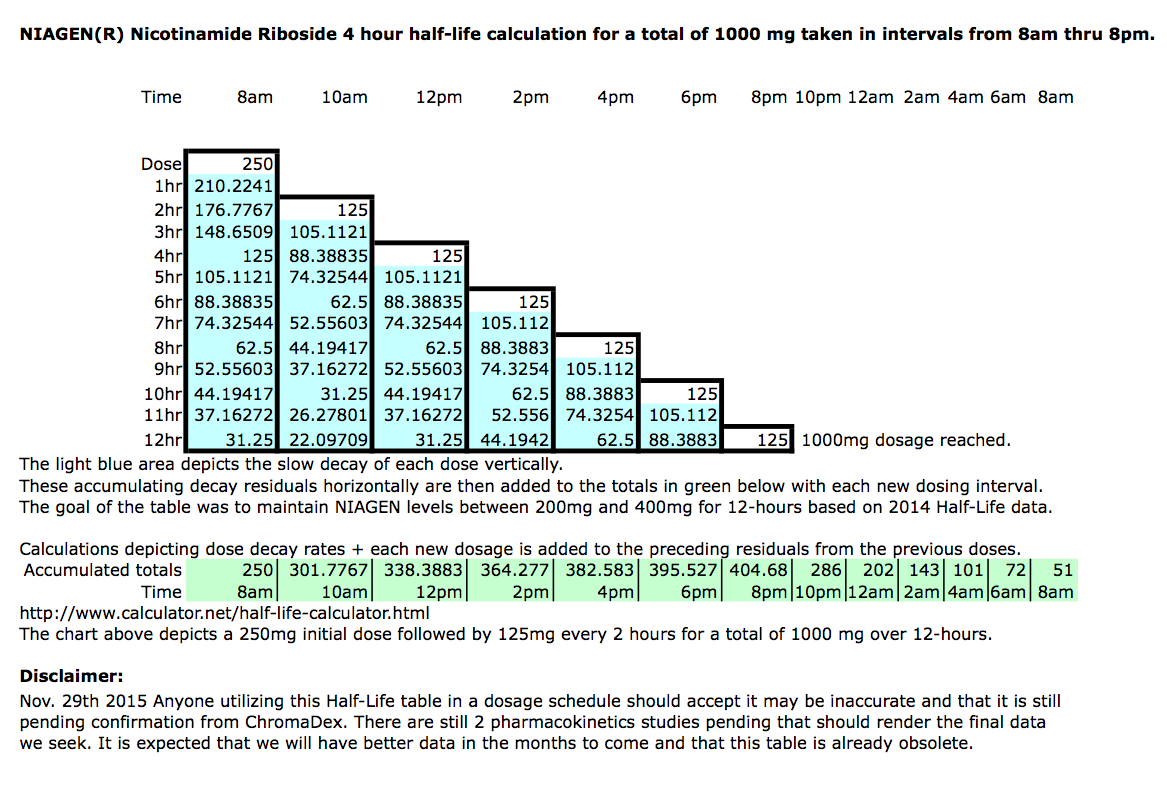
If last years 4-Hour-half-life data holds I already have a set of tables suggesting how often we might want to boost levels thru the day. Also they will be conducting long terms studies that will ask the question if the effectiveness of NR wanes with time. You see NR like all the other B3's is water soluble. As you consume a nutrient like this a certain amount of it is lost and excreted at a steady pace before it can do its intended job, so overdosing can waste money. The idea is to get as much as possible into the cells metabolic process without getting flushed down the drain. At some quantity a single mega dose starts to have diminishing returns because at those higher concentrations more is lost than can be utilized. So there is a theoretical dosing sweet spot where we would get the maximum NAD rise at the most economic rate.
I don't think any of us can afford to flush money down the drain.
Depending on the PK data released a time released Niagen product might be warranted but there isn't enough data to say if this will work.
I cant reliably interpret the released data for you so don't take me to task. My take is a ceiling was reached at a 300mg oral dosage and a 50% rise was averaged among the participants. Giving them 1000mg only increased the time they spent at the 50% NAD rise and that didn't push levels higher just for longer.
As far as the 2.7 fold comment I think this represents 170% above normal levels. I think this figure was one of the maximum results or best of from the group.
The Aarhus University Hospital study for the University of Copenhagen is completed but unpublished. They would not comment on the outcome and have not published. They still have more studies to go as you inferred but 2-human studies have already been completed. This is the data I seek.
The University of Colorado Boulder is the next big one I know of
http://www.colorado....volunteers.html
The one you mention "The company plans to initiate a placebo-controlled, double-blind, randomized study evaluating BASIS™ that will focus on overall quality of life with specific measures related to metabolic health. The trial will follow 120 people and Elysium Health plans to initiate it in the third quarter of 2015." So until its filed its flying under the radar. So far they haven't filed the paperwork.
Some of us already add Pterostilbene to our NR regiments. In fact you can put together everything in BASIS™ yourself for much cheaper. Here is a list of ChromaDex suppliers. http://www.pteropure...ucts/index.html
I'm one of those malcontents who believes 250mg's is inadequate to produce "much" therapeutic change. Its a supplement dose just scratching the surface. I think its better than taking nothing but I don't think based on the Na or NAM research we could expect all that much change in someones heath at such a low dose. Now this is my opinion and certainly open to argument. I think that NR has so much going for it as a calorie restriction mimic. It gets to work faster and doesn't take as many bodily resources to get to NAD. Its also the preferred cellular exchange precursor along with NaR and called to action at sites of injury.
I believe when this product first became available it was trialled at around 17 dollars per bottle as a "supplement." Given what was available in the market I thought this was slightly expensive but tolerable for what it represented. Then some months later David Sinclair shook the B3 space with his nicotinamide mononucleotide (NMN) findings. Keep in mind this is not nicotinamide riboside (NR) and as we've learned (NMN) is likely reduced to (NR) at the cell membrane anyway. But just the same David Sinclair is a headlines grabber and although the (NR) research had already demonstrated many of his (NMN) results it was 'his' results that resonated with the Media and Press and the headlines of rejuvenating muscle from a 60-year old state to a 20-year old state creating a ton of "Irrational exuberance."
I know all about Irrational exuberance. The master Louis Rukeyser explained the underpinnings of this state to me back in the 1980's. In the context of nicotinamide riboside (NR) it was close enough to nicotinamide mononucleotide (NMN) that people thought they could produce Sinclair's Lab results at home, on themselves. No one took into account the mega doses he used on the lab animals. So just like the Irrational exuberance that occasionally overwhelms the stock market and produces buying frenzies ChromaDex recognized they could get more for their new product with the hype Sinclair brought to the market. Being a publicly traded company this idea was good for shareholders and a new price point was determined with the buying frenzy Sinclair produced.
I still think they originally arrived at the proper price when Niagen was first introduced and it would now be more widely accepted at that price if they had not raised the price after the Sinclair hype. I think with the current price they've opened the door for the comparative/competitive research we're doing. If the pricing were more reasonable we wouldn't be looking at hybrid dosing with Na or Nam. So from a supplement standpoint I think its overpriced and the 250mg dose is insufficient, from a pharmaceutical standpoint it might be close to that value if it were marketed as a drug but as a supplement they are way off the mark.
So this is why I'm looking to get the most bang for the buck with the hybrid B3 approach.


































 This topic is locked
This topic is locked